Correctly selected music to lower blood pressure really helps to normalize the blood condition in patients with hypertension. This treatment method, although it has a good healing effect, is not able to fully replace antihypertensive medications and other components of complex therapy.
With a certain course of the disease, music therapy can only help in a situation if the patient follows other medical instructions. So, what melodies to listen to, how often, and why does listening to music normalize blood pressure?
The healing effect of music on blood pressure
Healing with music is one of the methods of modern art therapy, which has a gentle effect on the patient’s body, improves his health and accelerates the moment of relief from many diseases.
According to British scientists, if you listen to classical music for 30 minutes every day, this will help normalize blood levels and improve the well-being of patients with hypertension or hypotension. Medicine suggests that the therapeutic effect of musical art is explained by the fact that individual notes sound identically similar to the rhythm of the human body. While listening to calm music, the processes occurring in it with any deviations begin to adapt to its tone and gradually stabilize.
Experts believe that music relieves pressure:
- Calms
- Relaxes.
- Eliminates stress.
- Normalizes pulse.
- Regulates breathing.
- Relieves anxiety.
- Suppresses anxious thoughts.
- Stabilizes blood pressure.
- Improves blood circulation.
Classical music has a positive effect on brain activity, the autonomic nervous system and other structures of the body. In addition, there is a hypothesis that music therapy reduces the synthesis of the stress hormone cortisol.
Video: healing music for normalizing blood pressure
Video: High Blood Pressure Reduction Program
Music helps lower blood pressure much better than a salt-free diet or losing 5 kg of weight. Many cardiology centers examine the effect of various types of music on blood pressure and heart contractions:
- Rock.
- Pop music.
- Classic.
As the experiment showed, those hypertensive patients who listened to rhythmic youth music, their blood pressure rose by several units. In those patients who underwent music therapy with calm melodies, a decrease in blood pressure by 2-7 units was recorded. Of course, such indicators are quite modest, but these figures are quite enough to avoid the development of a hypertensive crisis, heart attack and cardiac complications.
As a result, the following conclusion was drawn:
| Types of music | How does it affect blood pressure? |
| Classical | Has a positive effect on the blood and heart. Significantly lowers blood pressure. Normalizes pulse. |
| Hard Rock | Surprisingly, in some cases it can lower blood pressure. |
However, not all Heavy-Metal works are capable of normalizing blood pressure; many of them have a completely opposite effect on the cardiovascular system.
Music that normalizes blood pressure, first of all, should be of the classical genre, doctors emphasize. It is advisable to listen to slow-tempo melodies that fade towards the end, for example, works by the composer Bach.
Music that lowers blood pressure is also useful for pregnant women who often have problems with blood pressure. Music therapy can also benefit patients during the rehabilitation period after stroke and heart surgery.
Listening to music 3 times a week for 15 minutes helps to significantly normalize blood pressure, and after 2 months of regular music therapy, not only stable dynamics are noted in relation to blood pressure, but also the general health of a person. After 4 months, arterial levels completely returned to normal limits.
Sleep and hypertension
home
/
To help the doctor
/
Sleep and hypertension
Sleep and wakefulness are two inseparable components of our life. And naturally, any pathological condition should also be viewed from this angle, i.e. assess the possibility of manifestation of the disease both while awake and during sleep. Wakefulness and sleep differ significantly from each other in many functional characteristics. Accordingly, it is logical to expect that the symptoms and manifestations of the disease may differ during the day and at night. In practice, when discussing the clinical picture of a disease, the doctor most often by default considers its manifestations in wakefulness, although in a dream the properties of the same pathological process may become different. On the other hand, when observing the development and course of various painful conditions, the possible modifying influence that processes directly associated with sleep have on them is often not taken into account.
The term “arterial hypertension” refers to the syndrome of increased blood pressure associated with hypertension (essential hypertension) and symptomatic arterial hypertension. Arterial hypertension in Russia remains one of the most significant medical and social problems. This is due both to the widespread prevalence of this disease and to the fact that arterial hypertension is the most important risk factor for major cardiovascular diseases, such as myocardial infarction and stroke, which mainly determine high mortality in our country. According to a survey conducted within the framework of the targeted Federal program “Prevention and Treatment of Arterial Hypertension in the Russian Federation,” the prevalence of arterial hypertension among the population in 2009 was 40.8% [1].
Arterial hypertension is one of the correctable diseases. However, poorly controlled hypertension remains an important cause of cardiovascular morbidity. Moreover, even a slight decrease in blood pressure results in a significant reduction in the number of often fatal complications. For example, a meta-analysis of studies on antihypertensive therapy showed that a decrease in systolic blood pressure by 10 mmHg. Art. or diastolic – by 5 mm Hg. leads to a reduction in the risk of heart attack by 22%, and stroke by 41% [2].
Sleep changes the functioning of the autonomic nervous system and other physiological parameters that can affect blood pressure. In addition, various sleep disorders can lead to a response in the form of transient episodes of increased blood pressure, which can increase the risk of arterial hypertension.
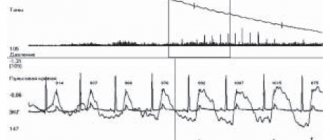
During normal sleep, blood pressure decreases compared to wakefulness. This effect is known as "dipping" and is partly due to the natural decrease in sympathetic tone during sleep. A decrease in both systolic and diastolic blood pressure during sleep by 10-20% compared to the waking period is considered normal. Accordingly, a decrease in blood pressure of less than 10% is inadequate and is called “non-dipping.”
The absence or insufficient reduction in blood pressure during sleep is a significant factor that independently increases the risk of developing cardiovascular complications. Thus, in a study by T. Ohkubo et al. (2000) showed that if the degree of insufficient reduction in blood pressure during sleep is only 5%, this already leads to an increase in cardiovascular mortality by approximately 20% [3], which is consistent with the results of studies by other authors.
It is known that the absence of a decrease in blood pressure during sleep is observed in many diseases, including most secondary arterial hypertension in kidney disease, diabetes mellitus and obstructive sleep apnea syndrome. A large number of studies have demonstrated that nocturnal blood pressure is a greater predictor of cardiovascular risk than waking blood pressure. Thus, in a study conducted in Dublin, more than 5000 patients with arterial hypertension were observed for the occurrence of various cardiovascular complications for 8 years [4]. The authors have convincingly proven that nighttime blood pressure readings are a more significant predictor of cardiovascular morbidity. Thus, according to the results of this study, an increase in nocturnal blood pressure of 10 mmHg. Art. led to an increase in cardiovascular mortality by 21%. Data from other similar studies also support the priority of nocturnal blood pressure in assessing the risk of cardiovascular consequences.
Summarizing the above data, we can conclude the following. On the one hand, even a seemingly insignificant decrease in blood pressure, especially during sleep, can significantly reduce the risk of the onset and progression of cardiovascular diseases. On the other hand, various diseases associated with sleep and, at first glance, unrelated to the pathology of the heart and blood vessels, through the mechanisms of increasing blood pressure, apparently can have a significant impact on cardiovascular morbidity and mortality.
There is a relationship between sleep duration and the risk of hypertension. Thus, in the Sleep Heart Health Study, it was shown that people who sleep less than 5 hours a day are significantly more likely to have arterial hypertension [5]. Similar results were obtained in the work of J. Gangwisch et al. (2006), who showed that sleep duration of less than 5 hours increases the risk of arterial hypertension by 60% [6]. It should be emphasized that such a dependence is not observed in the age group over 60 years [6, 7], which is probably due to differences in normal sleep duration for middle-aged and elderly people.
Another interesting feature noted by the researchers when analyzing the materials from the “Sleep Heart Health Study” was the fact that excess sleep is also not harmless and arterial hypertension is observed more often in those individuals whose sleep lasts more than 9 hours, compared to those sleeping 7-8 hours per day [5].
From the above, we can conclude that maintaining an adequate sleep and wakefulness regime is a significant component of the prevention and non-drug therapy of arterial hypertension, especially in middle age.
Insomnia (a similar but more familiar term for domestic specialists is insomnia) is one of the most common and clinically significant forms of sleep disorders. Insomnia is a sleep disorder characterized by complaints of difficulty falling asleep, insufficient sleep duration, intermittency or poor quality, despite the patient having sufficient time and opportunities for normal sleep, which leads to a deterioration in the quality of subsequent wakefulness.
Although chronic sleep disturbances in patients with insomnia are accompanied by increased levels of catecholamines and activation of the sympathetic nervous system, thereby predisposing to increased blood pressure, a number of researchers have questioned the existence of a relationship between insomnia and arterial hypertension [8], while other authors see a direct relationship between poor sleep quality and increases in both nighttime and daytime blood pressure [9]. An explanation of why insomnia is not always associated with the risk of increased blood pressure is contained in the work of J. Fernandez-Mendoza et al. (2012), which showed that insomnia is accompanied by an increased risk of arterial hypertension if it is associated with a shortening of total sleep time [10]. The risk of arterial hypertension in a patient with insomnia increases significantly only if the patient's sleep duration is less than 6 hours, which is consistent with our previously reported data on the role of sleep duration in the genesis of increased blood pressure. Based on the results of this study, the authors conclude that about half of patients with chronic insomnia have an increased risk of developing hypertension.
Insomnia appears to be less of an independent cause of hypertension in older people [11], which is again consistent with data on the effect of sleep duration on blood pressure in patients of older age groups. However, the practical experience of any doctor shows that complaints about the connection of poor sleep quality with episodes of increased blood pressure are common in elderly patients. This is also confirmed by the results of a study conducted under the leadership of Academician A.I. Martynov (2002), who revealed the relationship between sleep disturbances and increased blood pressure at night. It has been shown that older patients with hypertension and sleep disorders are 5 times more likely to have elevated nocturnal blood pressure. In addition, in patients with arterial hypertension and lack of normalization of nocturnal blood pressure during antihypertensive therapy, objective sleep indicators turned out to be significantly worse compared to patients with normal blood pressure values during sleep [12]. From our point of view, all the above data do not contradict each other. Apparently, the point is that insomnia is not an independent cause of symptomatic arterial hypertension in elderly patients, but it modifies and aggravates the course of the disease in patients who initially have high blood pressure.
The role of chronic insomnia in disrupting normal circadian rhythms of blood pressure is indirectly evidenced by the fact that treatment of patients with insomnia with modern non-benzodiazepine sleeping pills, simultaneously with improving sleep quality, leads to a decrease in blood pressure numbers, not only at night, but also during wakefulness [12, 13].
Non-benzodiazepine hypnotics include drugs that do not have a benzodiazepine element in their structure (a combination of benzene and diazepine rings), but exhibit affinity for the same parts of the inhibitory GABAA receptor complex that are also affected by benzodiazepines. These are the so-called Z-drugs - zopiclone (a cyclopyrrolone derivative), zolpidem (imidazopyridine) and zaleplon (pyrazolopyrimidine). The peculiarity of the action of these substances is the maximum affinity for the α1 subunit of the receptor complex, which is responsible for the hypnotic effect, with minimal affinity for the subtypes of subunits responsible for other, often undesirable effects of benzodiazepines. Compared to most available benzodiazepine hypnotics, Z-drugs have a fairly short half-life (from a minimum of 1 hour for zaleplon to a maximum of 5 hours for zopiclone). The drug with an average half-life is zolpidem (2.4 hours). It is recommended to take it in a dose of 10 mg immediately before bedtime for a course of no more than four weeks [14].
The dynamics of the daily blood pressure profile in elderly patients with arterial hypertension with sleep disorders while taking zolpidem were assessed in the work of L.I. Olbinskaya and B.A. Khapaeva (2000). It was shown that normalization of sleep during weekly administration of zolpidem is accompanied by an increase in the circadian index of systolic blood pressure, and in 3 out of 12 patients restoration of the normal diurnal blood pressure profile was observed [15]. In a recently published work by Y. Huang et al. (2012) these data were confirmed on a larger number of subjects in a placebo-controlled study: 103 patients with arterial hypertension and a non-dipper blood pressure profile received zolpidem for 30 days. In the group of patients who had poor sleep quality according to the Pittsburgh scale, there was a significantly greater number of transitions from the pathological non-dipper type to a normal decrease in blood pressure during sleep (11 out of 22 patients) than in the placebo group (2 out of 23 patients). At the same time, during treatment, a decrease in the level of circulating adrenaline and norepinephrine was noted. The authors concluded that the use of zolpidem for sleep disorders in patients with arterial hypertension is accompanied by improved sleep quality, a decrease in the severity of the stress reaction and normalization of the daily blood pressure profile [16].
In Russia, one of the most common zolpidem drugs is Sanval (Sandoz is a division of the Novartis group of companies, USA).
A connection has also been found between other types of sleep disorders and increased blood pressure. For example, this is observed in neurological disorders such as restless legs syndrome and periodic limb movements in sleep.
Restless legs syndrome is defined as a sensorimotor disorder characterized by severe discomfort in the limbs, which forces the patient to move them frequently, which interferes with the process of falling asleep or staying asleep. These sensations are rarely defined as “painful”; their peculiarity is that they intensify at rest and disappear with movement and walking. The severity of these symptoms increases in the evening and night and can significantly disrupt the process of falling asleep. In 80-90% of cases, restless legs syndrome is combined with periodic limb movements syndrome during sleep. The latter is characterized by the presence of characteristic, highly stereotypical motor episodes that are repeated during sleep, in which the legs are most often involved, which can also lead to sleep disturbance.
It has been shown that the presence of periodic movements of the limbs in a patient during sleep can cause an increase in his blood pressure. So M. Pennestri et al. (2007) in their study demonstrated that abnormal motor activity during sleep is accompanied in such patients by episodes of increased blood pressure, and the pressure increased to a greater extent in cases where movements provoked activation (micro-awakening) of the brain [17]. Having examined a group of patients with arterial hypertension, J. Espinar-Sierra et al. (1997) concluded that the incidence of periodic limb movements syndrome during sleep is directly related to the severity of arterial hypertension, and in patients with stage III arterial hypertension, abnormal motor activity during sleep occurs twice as often as in patients suffering from arterial hypertension I-II degrees [18]. In our opinion, this indicates, if not the possibility of periodic limb movements syndrome in sleep to independently lead to an increase in blood pressure, then at least its ability to aggravate the course of arterial hypertension in some of these patients. However, the work of L. Billars et al. is of greatest interest in this regard. (2007), who clearly demonstrated that the likelihood of arterial hypertension increases in proportion to the severity of periodic limb movement syndrome. Thus, the risk of increased blood pressure in the presence of more than 30 episodes of abnormal physical activity per hour of sleep, according to the authors, doubles [19].
A fairly large number of scientific studies have shown a connection between restless legs syndrome and arterial hypertension [20]. However, there are a number of studies that refute such a relationship [21]. A completely logical explanation for this contradiction from our point of view may be the fact that the vast majority of studies examining the relationship between restless legs syndrome and arterial hypertension were based on telephone interviews or questionnaire results. As a result, other significant factors might not have been taken into account and, in particular, the presence of periodic limb movements syndrome in the examined patients, which often accompanies restless legs syndrome, but requires a full-fledged polysomnographic study for its accurate diagnosis. In addition, it should be taken into account that the populations examined differed significantly, including in the age of the subjects. Thus, the risk of increased blood pressure in a patient with restless legs syndrome today should be classified as a probable hypothesis, for final confirmation of which additional research is required.
Obstructive sleep apnea syndrome (OSA) is characterized by repeated episodes of complete or partial obstruction of the upper respiratory tract (apnea and hypopnea), which are usually accompanied by a decrease in blood oxygen saturation and cause disruption of normal sleep patterns. The combination of loud snoring, pauses in breathing during sleep and excessive daytime sleepiness in one or another combination is observed in almost all patients and forms the clinical core of this syndrome.
Episodes of obstructive apnea cause fluctuations in systemic blood pressure - it gradually increases towards the end of the apnea and reaches its maximum when breathing resumes, after which it also gradually decreases. In this case, the value of blood pressure correlates with the severity of desaturation caused by apnea. Emerging disturbances in sleep structure also contribute to the increase in blood pressure following an episode of apnea [22].
A characteristic sign of OSA is the absence of a physiological decrease in blood pressure during sleep or even its increase during the night, and the severity of changes in the daily blood pressure profile largely depends on the severity of the patient’s respiratory disorders [23]. As a result, blood pressure in the morning may be higher than in the evening, even in the absence of antihypertensive therapy.
Arterial hypertension while awake occurs in more than half of patients with OSA and is observed in this group twice as often as in the general population. And although increased blood pressure is not necessarily a direct consequence of breathing disorders during sleep, and may be due to other reasons, such as gender, obesity or age, the presence of OSA has been shown to be an independent risk factor for arterial hypertension [24].
A typical component in the clinical picture of cardiovascular complications of OSA is systole-diastolic or predominantly diastolic arterial hypertension with fairly high blood pressure values, both in the morning and in the evening [25]. In this case, the value of blood pressure while awake largely depends on the severity of respiratory disorders during sleep.
Arterial hypertension in patients with OSA in some cases may be refractory to drug therapy [1]. Experience shows that even when it is possible to control blood pressure during the day, in some patients it is again significantly elevated when they wake up in the morning.
Correction of sleep apnea not only prevents nocturnal rises in blood pressure, but in some patients leads to an independent decrease in blood pressure during the daytime without additional prescription of antihypertensive drugs, which confirms the pathogenetic role of OSA in the genesis of arterial hypertension [26, 27]. Even if blood pressure while awake does not undergo significant changes, in patients with hypertension that is initially refractory to drug therapy, normalization of breathing during sleep often allows one to restore sensitivity to antihypertensive drugs. This effect must be taken into account when starting specific treatment for OSA in patients receiving blood pressure-lowering drugs at night, since such a combination can lead to severe nocturnal hypotension in them.
However, as mentioned above, in some cases, increased blood pressure may not be associated with respiratory disorders during sleep. Thus, we can conditionally divide patients with OSA and arterial hypertension into three groups [27]. The first includes patients with arterial hypertension, which is a direct consequence of severe obstructive breathing disorders during sleep. These are patients with nocturnal and morning arterial hypertension, which is to one degree or another refractory to drug antihypertensive therapy, but quickly disappears after elimination of OSA. It is in such patients that the value of blood pressure while awake is directly determined by the severity of breathing disorders during sleep. Usually these are relatively young patients with fairly severe OSA. The second, in our opinion, the most numerous group includes patients in whom OSA is only one of the causes of arterial hypertension. The last group consists of patients in whom arterial hypertension is not pathogenetically related to OSA and occurs as a result of some other causes. Correction of OSA in the latter does not lead to a decrease in blood pressure. Unfortunately, in many cases it is possible to definitively differentiate which group a particular patient belongs to only on the basis of treatment results. Therefore, in patients with clinically significant obstructive sleep apnea, treatment of arterial hypertension, by definition, should begin with normalization of breathing during sleep, which naturally does not negate the need for simultaneous administration of adequate antihypertensive therapy.
Arterial hypertension remains a pressing problem of modern clinical medicine, firmly retaining one of the key positions in the structure of causes leading to cardiovascular morbidity and mortality. The connection between hypertension and processes occurring during sleep is obvious, but still not sufficiently studied. Therefore, our task is to actively search and study the causes that contribute to the onset and progression of this disease, and to develop new approaches to its effective treatment.
LITERATURE:
- Chazova I.E., Ratova L.G., Boytsov S.A., Nebieridze D.V. Diagnosis and treatment of arterial hypertension. Recommendations of the Russian Medical Society on Arterial Hypertension and the All-Russian Scientific Society of Cardiologists // Systemic hypertension. 2010. No. 3. pp. 5-26.
- Law MR, Morris JK, Wald NJ Use of blood pressure lowering drugs in the prevention of cardiovascular disease: metaanalysisof 147 randomized trials in the context of expectations from prospective epidemiological studies // BMJ. 2009. Vol.338. P. 1245-1253.
- Ohkubo T., Hozawa A., Nagai K., et al. Prediction of stroke by ambulatory blood pressure monitoring versus screening blood pressure measurements in a general population: the Ohasama study // J. Hypertens. 2000. Vol. 18. P. 847-854.
- Dolan E., Stanton A., Thijs L., et al. Superiority of ambulatory over clinic blood pressure measurement in predicting mortality: the Dublin outcome study / Hypertension. 2005. Vol. 46. P.156 – 161.
- Gottlieb DJ, Redline S, Nieto FJ et al. Association of usual sleep duration with hypertension: the Sleep Heart Health Study / Sleep. 2006. Vol. 29. P.1009 – 1014.
- Gangwisch JE, Heymsfield SB, Boden-Albala B., et al. Short sleep duration as a risk factor for hypertension: analyzes of the first National Health and Nutrition Examination Survey // Hypertension. 2006. Vol. 47. P. 833-839.
- van den Berg JF, Tulen JH, Neven AK, et al. Sleep duration and hypertension are not associated in the elderly // Hypertension. 2007. Vol. 50. P. 585-589.
- Phillips B., Mannino DM Do insomnia complaints cause hypertension or cardiovascular disease? // J. Clin. Sleep Med. 2007. Vol. 3 P. 489-494.
- Olbinskaya L.I., Khapaev B.A. Sleep disturbances in patients with arterial hypertension are a possible risk factor and predictor of cardiovascular and cerebrovascular complications // Cardiology. 1999. No. 6. pp. 18–22.
- Fernandez-Mendoza J., Vgontzas AN, Liao D., et al. Insomnia with objective short sleep duration and incident hypertension: the Penn State Cohort // Hypertension. 2012. Vol. 60. P. 929-935.
- Phillips B., Bůzková P., Enright P. Cardiovascular Health Study Research Group. Insomnia did not predict incident hypertension in older adults in the cardiovascular health study / Sleep. 2009. Vol.32. P. 65-72.
- Martynov A.I., Vein A.M., Ostroumova O.D. and others. The use of zopiclone for the correction of high blood pressure in the sleep-wake cycle in elderly patients with essential arterial hypertension and insomnia // Cardiology. 2002. No. 8. pp. 11-14.
- Deruzhinskaya N.A., Syropyatov O.G., Selyuk M.N. and others. The use of somnol as an adjuvant agent in the treatment of insomnia in arterial hypertension // Medical news. 2009. No. 5. pp. 55-58.
- Sanval®: instructions for use, contraindications, composition and price, 3D packaging. Electronic document https://www.rlsnet.ru/tn_index_id_9929.htm as of 03/03/2013.
- Olbinskaya L.I., Khapaev B.A. Combined use of zolpidem and enalapril in elderly people with essential arterial hypertension and sleep disorders / Clinical Medicine. 2000. No. 9. pp. 47-50.
- Huang Y., Mai W., Cai X. et al. The effect of zolpidem on sleep quality, stress status, and nondipping hypertension / Sleep Med. 2012. Vol. 13. P.263-268.
- Pennestri MH, Montplaisir J, Colombo R, et al. Nocturnal blood pressure changes in patients with restless legs syndrome // Neurology. 2007. Vol.68. P. 1213-1218.
- Espinar-Sierra J., Vela-Bueno A., Luque-Otero M. Periodic leg movements in essential hypertension // Psychiatry Clin. Neurosciences. 1997. Vol.51. P. 103-107.
- Billars L., Hicks A., Bliwise D., et al. Hypertension risk and PLMS in restless legs syndrome // Sleep. 2007. Vol. 30 (suppl). A297-A298.
- Ulfberg J., Nystrom B., Carter N., Edling C. Prevalence of restless legs syndrome among men aged 18 to 64 years: an association with somatic disease and neuropsychiatric symptoms // Mov. Discord. 2001. Vol.16. P. 1159-1163.
- Högl B., Kiechl S., Willeit J., et al. Restless legs syndrome: a community-based study of prevalence, severity, and risk factors // Neurology. 2005. Vol. 64. P. 1920-1924.
- Shepard JW Hemodynamics in obstructive sleep apnea // Abnormalities of Respiration During Sleep. Orlando: Grune and Stratton, 1986, pp. 39-62.
- Kalinkin A.L. The role of sleep apnea syndrome in the course of hypertension: Dis. ...cand. honey. Sci. – M., 1997.
- Nieto FJ, Young TB, Lind BK et al. / Prospective study of the association between sleep-disordered breathing and hypertension / JAMA. 2000. Vol.283. P.1829-1836.
- Poluektov M.G. Obstructive sleep apnea syndrome and other breathing disorders during sleep in adults / Somnology and sleep medicine. Selected lectures (edited by Ya.I. Levin and M.G. Poluektov). M.: Medforum, 2013. pp. 221-232.
- Voronin I.M. Cardiovascular consequences of obstructive breathing disorders during sleep. Tambov: Publishing house of TSU named after. G.R. Derzhavina, 2001.
- Sumarokov A.V., Palman A.D., Danilyak I.G. Blood pressure in patients with sleep apnea syndrome and its dynamics during treatment // Russian Medical News. 1998. No. 2. pp. 61-64.
What music is good for cardiovascular and related ailments?
Despite the fact that there is controversy surrounding music therapy about its ability to heal many diseases, medical practice confirms that the works of famous composers can be used to treat quite serious pathologies.
Listening to them in a certain tone helps speed up the healing of certain organs and structures of the body that correspond to a given tone. Let's consider what healing music is suitable for normalizing blood pressure and eliminating certain pathologies:
| Pathologies and conditions of the body | What to listen to |
| To improve mood and relieve depression | Bizet's "Habanera" (from the opera "Carmen"). Verdi's "Triumphal March" (from the opera "Aida"). Mozart "Rondo in the Turkish Style". |
| Ophthalmological disorders | D flat major (Chopin's Nocturne). |
| Otitis Tonsillitis Pathologies of the vertebrae of the neck | E flat major (Liszt Piano Concerto). |
| Anxiety Indecisiveness | Strauss "Waltzes". Chopin "Mazurka". Rubinstein "Melody". |
| Hypertension Tachycardia | Preference is given to works that have a slow tempo, for example: Mendelssohn’s “Wedding March”. Bruckner "Mass in A Minor". Bartok "Piano Sonata". Chopin "Nocturne in D minor". “Concerto in D minor” for violin (Chopin Cantata 21). |
| Insomnia | Sibelius "Sad Waltz". Grieg "Peer Gynt" Glitch "Melody". Schumann "Dreams" Plays by Tchaikovsky. |
| Migraine | Mendelssohn "Spring Song". "Gershwin and Dvorak" Humoresques ". |
| Headache due to nervous tension | Beethoven "Fidelio". Khachaturian "Masquerade". Mozart "Don Giovanni". Oginsky "Polonaise". Liszt "Hungarian Rhapsody". |
| Overwork | E. Presley. L. Armstrong. D. Wellington. |
| Heart and blood vessels Pathologies of the respiratory system | F sharp minor (Preludes and Fugues, volume 1 HTC Bach). |
| To improve the composition of blood fluid Spinal pathologies | “Ave Maria” by Schubert (A sharp minor) in several variations: The first is “Ave Maria” (Schubert). The second is “Ave Maria” (Schubert). The third is “Ave Maria” (performed by S. Shirshebo). The fourth is “Ave Maria” (performed by L. Pavarotti). |
| Kidney failure Bladder abnormalities | D major (Waltz “Blue Danube” by Strauss). |
| Edema Varicose veins | A major (Beethoven's Kreutzer Sonata). |
| Arthritis Joint problems | B major (Preludes and Fugues, volume 1, HTC Bach). |
| Hypotension | Low blood pressure music should have an energetic tempo. |
In addition to certain melodies, specific musical instruments also improve well-being:
- Drum - brings closer the moment of healing from blood vessel defects and heart pathologies.
- Harp - has a healing effect on the condition of the heart.
- Violin – relieves mental pain and worries.
- Flute – cures lung ailments.
- Saxophone – increases sexual energy.
- Piano – helps with thyroid diseases.
- Organ – strengthens the spine, clears the mind of negative thoughts.
As to whether music therapy has any contraindications, it does not have any; the main thing is to choose the right melody correctly.
Rules for music therapy for problem blood pressure
In order for music therapy at home for hypertension or low blood pressure to be effective, you should follow the rules for its use:
- Before you turn on the music, you need to create a favorable atmosphere in the room.
- It is advisable to listen to it alone, so that no one disturbs your musical relaxation session.
- You can't be distracted while listening.
- Music recording must be of high quality.
- Music therapy can be combined with a healing bath.
- When choosing a melody, listen to your intuition - it should please you and evoke positive feelings.
- If a piece of music evokes negative emotions, you should not continue listening to it.
- You need to listen to music or a song in a comfortable position, preferably with your eyes closed, as if letting it pass through you.
- Try not to be distracted by extraneous thoughts; music should completely fill your mind and thoughts.
- The sound volume should not be strong. The healing melody should sound quietly, so you should not turn it on “at full blast”.
- Keep it in moderation. The first music therapy sessions should not last more than 10 minutes, and subsequently their duration is increased to 30 minutes.
High blood pressure after waking up: causes and dangers
If in the morning after waking up you feel lethargic and there are cobwebs in front of your eyes, the tonometer is guaranteed to show high numbers. Regular manifestation of symptoms is a reason to consult a doctor. Based on the research, he will conclude:
- genetic predisposition to hypertension;
- the need to combat excess weight;
- prescribing a course of treatment for cardiovascular diseases;
- hormonal adjustments.
The main reason for morning jumps is the body’s transition from the sleep phase to the active phase. Different hormones are responsible for wakefulness and rest. A person maintains a balance of substances, but one of the elements may become more or less. A person’s condition in the morning is also influenced by the environmental factor before or during sleep. A large feast with libations, stress at work or at home can be reflected at night in the form of insomnia, severe headache, which is certainly reflected in the tonometer readings.
The risk of an increase in the morning increases when the patient reaches 50 years of age and abuses alcohol, drugs and tobacco. Due to the poisoning of the body, the patient experiences more severe consequences of cerebral hemorrhages and heart attacks.
What music lowers blood pressure
The positive effect of music on the body has been noted and proven in the works of scientists from all over the world. They distinguish several categories of music for high blood pressure. In first place in importance are the classical works of Chopin, Mozart and other outstanding composers. This is music that reduces blood pressure due to the predominance of a frequency range that is safe for humans and the measured tempo of the melody.
Hard rock, beloved by young people, does not have such an effect. The melodies are dominated by high frequencies, and the musicians sing using ultrasound. Constant contact predictably keeps a person stressed, which is reflected in the morning state after attending a concert. There are frequent cases of such music being used to commit murder in absentia.
In the treatment of hypertension, meditative relaxation programs are popular, where therapeutic melodies can be combined with calming videos. It is recommended to listen to them through stereo headphones. During the session, it is recommended to step away from current problems and be alone with yourself. The main thing is to listen to the song for lowering blood pressure with faith in a miracle.