What is pancreatitis
Pancreatitis is inflammation of the pancreas. This organ secretes enzymes into the duodenum (just behind the stomach) that help food digest, such as amylase (to break down carbohydrates) and lipase (to break down fats). With severe inflammation of the pancreas - acute pancreatitis - its cells are destroyed and enzymes enter the blood. Therefore, for any severe abdominal pain, doctors determine the level of amylase in the blood.
Acute pancreatitis is a painful and very dangerous disease. Its symptoms are almost impossible to endure “on your feet”: it is a severe, persistent pain in the pit of the stomach and under the left rib, which often radiates to the back (so-called girdling pain occurs). A person with acute pancreatitis often even takes a special position on the bed - lying on his left side, so as not to increase the pain by moving the ribs when breathing. Most people with acute pancreatitis experience severe nausea and vomiting; any food intake increases the pain: after all, the pancreas begins to secrete enzymes when eating, and this increases blood flow, and therefore pain. Many people's body temperature rises.
Diagnosis of acute pancreatitis is the job not so much of gastroenterologists as of surgeons, since the intensity of pain can be the same as with appendicitis and other “surgical” pathologies.
Symptoms of pancreatitis in men and women
From a physiological point of view, the pancreas is a very important organ of our body, responsible for normal digestion, as well as the production of the hormone insulin. A lack of the latter can cause diabetes.
In acute pancreatitis, the symptoms are similar to severe poisoning. This happens because during inflammation, enzymes are retained inside the pancreas, causing its subsequent destruction. Dead cells enter the blood in large quantities, which is manifested by symptoms of intoxication.
The most common signs of acute pancreatitis are described as follows:
- Intense constant cutting or dull pain that does not go away for a long time (up to painful shock). Pain is felt under the ribs on both sides (together or separately), sometimes pain is felt throughout the entire area of the abdomen and radiates to the lumbar region.
- A sharp decrease or increase in blood pressure.
- Changes in complexion: with pancreatitis in children and adults, the skin turns pale, gradually approaching grayish shades.
- Increase in body temperature to high levels.
- Nausea, hiccups, belching, and a feeling of dry mouth. Vomiting with secretion of bile.
- Diarrhea (diarrhea) with pancreatitis is a common phenomenon. Moreover, the feces come out with foam, with a sharp unpleasant odor, and undigested pieces of food are noticeable in it. There may also be constipation.
- Abdominal muscle tension.
- The appearance of shortness of breath, a characteristic icteric coating on the tongue, as well as sticky sweat: all this is the result of a lack of electrolytes due to vomiting and diarrhea.
- Bloating.
How does acute pancreatitis occur?
About 70% of all cases of acute pancreatitis are due to either alcohol poisoning or gallstones. Excessive alcohol consumption (even without a history of alcoholism) causes inflammation of the pancreas. For the same reason, people who systematically abuse alcohol have every chance of not only ending up in the hospital with severe acute pancreatitis, but also experiencing pain attacks again for many years. A gallstone can also cause pancreatitis: the duct that carries bile from the bladder into the duodenum merges with the pancreatic duct. This situation - biliary pancreatitis - requires emergency intervention, for example, to dissect the large duodenal papilla: this is the place where the ducts flow into the intestine.
Acute pancreatitis can also be caused by the toxic effects of certain medications, trauma to the gland during surgery, or high levels of fat in the blood. It is extremely rare and, as a rule, in the presence of other similar diseases, the pancreas becomes inflamed due to the excessive action of the immune system on it.
Whatever the cause of the onset of the disease, acute pancreatitis is always accompanied by abdominal pain. You should not assume this diagnosis if you feel unwell from a medicine or some product.
Our services
The administration of CELT JSC regularly updates the price list posted on the clinic’s website. However, in order to avoid possible misunderstandings, we ask you to clarify the cost of services by phone: +7
| Service name | Price in rubles |
| Ultrasound of the abdominal organs (liver, gall bladder, pancreas, spleen) | 3 800 |
| Pancreatocholangiography | 4 500 |
| MSCT of the abdominal cavity and retroperitoneal space of the abdomen | 6 000 |
All services
Make an appointment through the application or by calling +7 +7 We work every day:
- Monday—Friday: 8.00—20.00
- Saturday: 8.00–18.00
- Sunday is a day off
The nearest metro and MCC stations to the clinic:
- Highway of Enthusiasts or Perovo
- Partisan
- Enthusiast Highway
Driving directions
Acute pancreatitis has been dealt with. What about chronic?
If the toxic effect on the pancreas does not stop (for example, a person continues to drink excessively) or the organ was very damaged during the first (acute) episode of pancreatitis, the pain returns again and again.
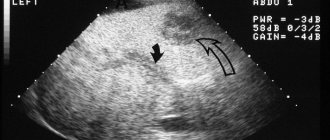
During exacerbations of chronic pancreatitis, blood tests may remain normal. But over time, external signs may appear, which doctors detect by examining the pancreas using ultrasound (ultrasound), X-rays (CT or computed tomography) or magnetic resonance imaging (MRI). These are narrowing of the pancreatic ducts, the appearance of compactions in it - calcifications, as well as the appearance of cysts - bubbles with liquid in place of dead tissue. An examination for suspected chronic pancreatitis is carried out with another important goal - not to miss pancreatic cancer, which may initially be accompanied by the same symptoms.
With constantly renewed inflammation of the pancreas, its function—the secretion of enzymes that digest food—is disrupted over time. As a result, a person is bothered by constant bloating, diarrhea, and the stool becomes greasy (for example, it is difficult to flush from the toilet). This condition - exocrine insufficiency - is most conveniently identified by determining the content of pancreatic elastase (a pancreatic enzyme) in the stool.
Diagnostics
It is a very difficult matter, but when stones are visible in the projection of the pancreas during an X-ray of the abdominal cavity, this is considered sufficient to make a diagnosis. But ultrasound is not used to detect chronic pancreatitis because it is not informative; the gland is not visible at all.
CT helps to make a diagnosis and monitor changes in the pancreas, but MRI is much worse in quality.
Endosonography is the same sensitivity as CT - a combination of endoscopy and ultrasound, plus you can immediately take a puncture from the gland. If the instrumental examination is uncertain, functional tests can be performed that indirectly assess the working capabilities of the organ in the later stages, when secretory insufficiency has flourished, but their information content leaves much to be desired.
How to treat chronic pancreatitis
In general, the goal of treating chronic pancreatitis is to eliminate pain. Anti-inflammatory drugs, such as paracetamol, are used for this. Enzymes are often prescribed to people with chronic pancreatitis. Unfortunately, this does not always relieve pain. Previously, it was assumed that adding enzymes to food would reduce the load on the pancreas - it would not have to secrete its own enzymes. In reality, everything is not so simple: the secretory (excretory) activity of the gland depends on completely different substances - hormones, for example secretin. Their production is more influenced by the fat content of food and the regularity of its intake than by the content of drug enzymes in the intestine. Nevertheless, enzymes for chronic pancreatitis are necessarily prescribed (often for life) if there are signs of poor secretion of one’s own enzymes (bloating, loose stools). Enzymes are always drunk directly with food: “between spoons.” For the same reason, it is illiterate to prescribe taking enzymes “so many times a day.” It is more correct to warn a person with the disease that the drug should be carried with them and taken with any food intake.
A diet for chronic pancreatitis alleviates the course of the disease, although it is difficult to accurately determine the list of possible products the first time. You definitely shouldn't drink alcohol, but traditionally it is recommended to eat less fatty foods and snack more often, giving preference to slow carbohydrates - fruits and vegetables. Cooking exclusively by steaming is not the most proven way to alleviate pancreatitis; it is much more important not to overindulge in very spicy foods. Roughly speaking, there will most likely be no harm from a chicken cutlet, even fried without much seasoning.
The main thing in the treatment of chronic pancreatitis is to remove the cause of the disease.
If a person suffers from alcoholism or smokes, refer him to a narcologist (smoking itself does not cause pancreatitis, but increases exacerbations). If pancreatitis occurs due to gallstones, remove the bladder. If fat metabolism is disturbed in the body, consult a cardiologist and select treatment with drugs that reduce the level of lipoproteins and triglycerides, and select a diet.
Preventive measures
To avoid increased blood pressure during pancreatitis, it is recommended:
- Compliance with a dietary diet (exclusion from the menu of high-calorie, spicy and salty foods).
- Regularly engage in accessible sports and breathing exercises.
- Stay in the fresh air every day (at least 1 hour a day).
For patients with symptoms of pathology, it is equally important to quit smoking and get enough sleep. Avoid stress, minimize the consumption of alcohol, strong tonic drinks - coffee and black tea.
Conservative treatment
The goal of conservative treatment of patients with CP is to relieve symptoms and prevent the development of complications. There are 6 main objectives that must be achieved [2]:
1. Stop drinking alcohol and quit smoking.
2. Determining the cause of abdominal pain and trying to reduce its intensity.
3. Treatment of insufficiency of exocrine pancreatic function.
4. Detection and treatment of endocrine insufficiency in the early stages before complications develop.
5. Nutritional support.
6. Screening for pancreatic adenocarcinoma, especially in hereditary pancreatitis.
Behavior change (lifestyle modification) and nutritional therapy
Complete abstinence from alcohol consumption is recommended to reduce the incidence of serious complications and mortality. In addition, in conditions of abstinence, in some cases, a decrease in the severity of symptoms and relief of pain was noted, while continued alcohol consumption contributes to the progression of the disease [1, 2, 15]. Exocrine pancreatic insufficiency, as a rule, does not progress with abstinence from alcohol consumption [15]. Individuals who do not drink alcohol have a better response to pain management therapy [15–22]. However, stopping drinking alcohol does not always stop the progression of the disease. To stop drinking alcohol, it is necessary to involve narcologists and psychiatrists specializing in alcohol dependence, followed by the supervision of a psychologist [2].
In general, it is very difficult to identify the role of smoking in alcohol abuse as an etiological factor and a factor influencing the course of CP, since smoking often accompanies alcohol abuse [8, 23–30]. In addition, abstinence from alcohol consumption is often not associated with smoking cessation [1]. Retrospective data indicate the beneficial effects of smoking cessation in reducing/preventing pain and complications in CP [31, 32]. In any case, patients with CP are recommended to quit smoking as a significant and independent factor in the development of CP [16, 32].
Protein-energy malnutrition is common among patients with CP, and is multifactorial in nature due to abdominal pain syndrome, malabsorption, diabetes mellitus (DM), impaired intestinal motility and chronic alcoholism [33]. From the standpoint of science, based on evidence, there is no specific “diet for CP”, and we only have empirical experience in using the familiar “gentle nutrition”, or “table No. 5p”, which is familiar to everyone. In general, these recommendations boil down to eating low-fat, high-protein, and high-carbohydrate meals in smaller portions, especially for patients with steatorrhea. The degree of fat restriction is thought to depend on the severity of malabsorption. Patients usually tolerate a pure fat intake of <40–60 g per day. Specific recommendations include a daily energy diet of 2500–3000 calories, protein intake of 1.0–1.5 g/kg/day, and a fat intake of <30–40% of daily calories [2, 33]. However, there is no official data based on the results of randomized trials indicating the need to reduce fat intake in patients with pancreatogenic steatorrhea [1]. It is extremely important to remember that switching to a low-fat diet is challenging and can impair nutritional balance and lead to decreased vitamin levels. Since there have been no specific studies examining macronutrient intake patterns that can prevent the development of isolated complications of CP, it can be assumed that complex carbohydrates and dietary fiber may be useful in slowing the rate of development of diabetes.
Patients with CP may experience impaired absorption of fat-soluble vitamins (A, D, E and K) [1], which is accompanied by a decrease in their concentration in the blood serum [34]. However, clinical manifestations of hypovitaminosis rarely appear [2, 35–37]. Therefore, persons with uncontrolled exocrine pancreatic insufficiency and/or a long history of CP (more than 5 years) require biochemical screening of fat-soluble vitamins, and if they are reduced, parenteral administration of fat-soluble vitamins [1].
Patients with CP may develop deficiency of vitamin B12, which is absorbed in the terminal ileum and forms a complex with intrinsic Castle factor. When vitamin B12 enters the stomach, it binds to haptocorrin (R-protein, or Castle factor). Haptocorrin is broken down in the small intestine by pancreatic enzymes, thereby releasing B12. In patients with pancreatic dysfunction, vitamin B12 may remain bound to haptocorrines and not be absorbed in the terminal ileum. Patients who continue to abuse alcohol are also at risk of developing thiamine (vitamin B1), riboflavin (vitamin B2) and pyridoxine (vitamin B6) deficiencies. If insufficient levels of vitamins in the blood serum are detected, vitamin replacement therapy should be carried out.
Osteoporosis is an established complication of CP; It is recommended to perform a one-time assessment of bone mineral density (using X-ray densitometry) [37].
Treatment of abdominal pain syndrome
Pain is the most common and most significant symptom in CP. The mechanism of pain is not precisely established and is likely multifactorial; additional examination is often required to establish it [4].
Factors that determine the development of pain in CP include [2]:
• formation of false cysts;
• stenosis of the duodenum (DU);
• strictures of the biliary tract;
• pancreatic cancer;
• other concomitant diseases (for example, peptic ulcer).
If the above factors are excluded, consistent conservative treatment is carried out [2]. Despite the fact that pain in CP may subside over time, especially in alcohol-related pathology, its duration cannot be predicted [38]. Initial therapy consists of periodic or course use of simple non-narcotic analgesics (paracetamol or non-steroidal anti-inflammatory drugs - NSAIDs) along with a low-fat diet. The drugs should be taken 30 minutes before meals to minimize postprandial pain [1, 2].
In Russia, the recommendations of a number of foreign associations [1–5] on trial replacement therapy with high doses of pancreatic enzymes for 6 weeks (in the form of tablets without a protective coating) [4, 38–40] are not available for implementation due to the lack of such drugs on the pharmacological market in Russia . However, there is insufficient evidence of the effectiveness of such therapy in controlled studies [1, 2].
A possible mechanism for pain relief with enzyme replacement therapy (ERT) is to reduce the stimulation of the pancreas by cholecystokinin released in response to food intake. When exogenous pancreatic enzymes enter, releasing factors undergo proteolysis, which leads to a decrease in the release of cholecystokinin in response to food intake, a decrease in the secretory tension of the pancreas and, accordingly, pain. Clinical trials examining the validity of this hypothesis have yielded conflicting results [39, 40]. Enteric-coated tablet pancreatin, registered in Russia, has no evidence of effectiveness at all, since it has not been tested in any placebo-controlled study.
In studies using non-enteric-coated tablets, a decrease in pain was observed compared with placebo. It should be remembered that the effects of drugs based on pancreatic enzymes without a protective coating were enhanced by therapy that suppresses acid production (H2 blockers or proton pump inhibitors), which prevents the inactivation of enzymes under the influence of acid in the stomach and increases the level of proteases reaching the duodenum [ 38, 41]. When combining microtablets or minimicrospheres of pancreatin, coated with an enteric coating, with antisecretory drugs, early opening of the membranes and activation in the initial parts of the duodenum are possible, where the principle of negative feedback can be implemented. There are no experimental studies confirming this hypothesis, but there are individual randomized [42] and non-randomized [43] studies that indirectly confirm this fact, which has long been reflected in the practice of Russian gastroenterologists and surgeons.
It is assumed that ERT for CP with pain is most effective in the absence of duct dilatation or with minimal changes in the pancreatic parenchyma [44]. Octreotide is also effective in suppressing pancreatic secretion, but currently it is not recommended for use in the treatment of chronic pain [38] due to the ambiguity of the available scientific data and the impossibility of long-term use (high cost, adverse events) [2].
Patients with persistent pain may require the use of narcotic analgesics [1,2] due to the lack of effectiveness of NSAIDs [23, 29, 45–48]. It is believed that tramadol should be initially preferred over morphine due to its less pronounced effect on the functions of the gastrointestinal tract [48]. Narcotic analgesics in different dosage forms have similar effectiveness [46]. You should start with drugs with the least activity, followed by a transition, if necessary, to potent drugs. Initially, it is recommended to prescribe narcotic analgesics only as needed (as required for severe pain). In general, regular use of opioids is only required when endoscopic or surgical treatments fail and symptoms persist [2].
Tricyclic antidepressants reduce the manifestations of concomitant depression, can reduce the severity of pain and potentiate the effect of analgesics. These drugs can change the sensitivity of the central nervous system and visceral nerves, the role of which is assumed in the development of pain in CP [2, 44].
Chronic intake of antioxidants may be effective in preventing attacks of pain in CP [1]. Only one randomized controlled trial has demonstrated the effectiveness of oral antioxidants (selenium, beta-carotene, ascorbic acid, tocopherol, and methionine) as adjunctive therapy for the prevention of attacks of pain. Overall, antioxidant supplementation resulted in a significant reduction in the number of pain days per month, a reduction in the need for oral analgesics, and a reduction in hospitalizations. By the 3rd month, a statistically significant beneficial effect of antioxidants on pain relief was already noted [49]. The results of this study require confirmation [1, 2] to adapt such tactics to routine clinical practice.
Treatment of pain in CP should be carried out jointly with qualified surgeons and endoscopists who can offer minimally invasive techniques for relieving/reducing pancreatic pain (blockades, stenting, etc.) and/or surgical treatment.
Treatment of insufficiency of exocrine function of the pancreas
Clinically significant impairment of the absorption of fats and proteins occurs only when the functional activity of the pancreas decreases by more than 90% [38]. Steatorrhea usually precedes protein deficiency [38] and occurs in the late stages of CP (approximately 50% of patients, on average 10–12 years after the onset of the disease) [50]. It may be more common than previously thought [51]. The main clinical consequences of CP are wasting and steatorrhea caused by impaired fat digestion [52].
Pancreatic enzyme replacement therapy improves fat absorption in patients with CP and exocrine pancreatic insufficiency [53] and can normalize nutritional status, such as the level of fat-soluble vitamins, prealbumin and ferritin, including in patients without overt steatorrhea [50, 52] , prevent the development of osteoporosis caused by vitamin D malabsorption [36, 37].
Indications for PRT [2]:
• severe steatorrhea;
• weight loss;
• diarrhea;
• long-term course of CP (more than 5 years of history) [1, 51].
Adequate and timely treatment helps to avoid the development of serious complications and reduce mortality due to malnutrition.
For patients with clinically significant steatorrhea (unformed, greasy, foul-smelling stool in large quantities), it is possible to prescribe pancreatic enzymes only on the basis of clinical data [1]. In CP with signs of nutritional deficiency (weight loss, muscle wasting, osteoporosis, signs of hypovitaminosis), ERT can be indicated even without diagnosing steatorrhea using the method of quantitative assessment of excreted fat and normal stool appearance [1, 51].
A standard coprological study with the detection of neutral fat is characterized by low sensitivity, therefore, when using it to verify steatorrhea and evaluate its effectiveness, it is necessary to carry out the test three times and take into account the patient’s diet and stool frequency. A 72-hour stool collection to determine the fat absorption coefficient (neutral fat quantification), although the gold standard for diagnosing steatorrhea, is used only in clinical trials [50].
Minimicrospheres containing the pancreatin enzyme are coated with an enteric coating (Creon). They are much more effective than any tablet drugs in the treatment of steatorrhea, since lipase is not inactivated in the stomach by acid. Thus, improved pharmacokinetics results in a more likely contact of enzymes with chyme and a larger contact area [54]. Minimicrospheres with a diameter of 1.0 to 1.2 mm are evacuated simultaneously with food. Their effectiveness is 25% higher compared to microtablets measuring 1.8–2.0 mm [52, 55].
Thus, the prediction of the effectiveness of TRT will definitely be influenced by the choice of drug. It is important to remember that in different pancreatin preparations the content of lipase, protease and amylase is not the same. The patient should receive at least 25–40 thousand units of lipase for the main meal and 10–25 thousand units of lipase for an intermediate meal [1, 2, 56], which should be at least 100 thousand units per day.
Treatment usually results in clinically significant weight gain and symptomatic relief.
Serological (retinol binding protein, transthyretin) and general clinical (absolute lymphocyte count in the absence of other causes of lymphocytopenia) markers can be used to monitor nutritional status. The use of an average of 40 thousand units of lipase per meal for one year leads to normalization of fat absorption, a significant increase in body weight, normalization of the level of retinol-binding protein and prealbumin in the majority of patients with CP [50]. For patients with no effect of treatment, laboratory methods for assessing fat absorption can be used - dynamic determination of neutral fat in the stool and C13 breath tests [35, 50]. Despite clinical improvement, malabsorption may persist in some patients, which requires the use of higher doses of Creon (up to 60 thousand lipase units per meal or more) [50].
Patients with persistent symptoms despite taking high doses of enteric-coated enzyme preparations should be prescribed therapy that suppresses acid production [54], due to a sharp decrease in bicarbonate secretion in the pancreas with insufficient neutralization of chyme acidity in the duodenum [52, 57]. The preferred drugs are proton pump inhibitors in standard doses [1, 2], which are prescribed only for persistent steatorrhea. With persistent steatorrhea, it is necessary to exclude other causes of diarrhea, in particular those associated with bacterial overgrowth in the small intestine, which often occurs in CP [58], protozoal infections, and celiac disease.
Adequate replacement therapy with Creon significantly improves the quality of life of patients with newly diagnosed and never treated CP and patients who received FPP in insufficient doses. A significant relationship has been established between improvements in quality of life indicators and body weight or a decrease in the excretion of fat in feces [59].
Long-term treatment with pancreatic enzymes in daily doses of up to 200 thousand units of lipase is absolutely safe, as evidenced by the results of numerous studies of children with cystic fibrosis, adult patients with CP and those who underwent extensive resections of the pancreas [60]. At the same time, a common misconception among patients and doctors is the so-called. harm of long-term treatment with pancreatic enzymes. There are no scientific explanations for this assumption. It is based only on the opinion expressed by someone unknown about “addiction of the pancreas,” “atrophy of the pancreas,” and the fact that “your pancreas will stop working altogether.” On the one hand, studies conducted in which extremely high pancreatin levels were used (360 thousand units of lipase per day) did not show any effect on pancreatic secretion [61]. On the other hand, leaving a CP patient with pancreatic insufficiency without vital replacement therapy is criminal and tantamount to canceling replacement therapy with levothyroxine, antihypertensive and hypoglycemic drugs for hypothyroidism, arterial hypertension and diabetes, respectively.
Treatment of endocrine insufficiency
70% of patients with CP develop impaired glucose tolerance over time. The likelihood of endocrine insufficiency begins to gradually increase 10 years after the onset of the disease [38]. Pancreatogenic diabetes differs from diabetes types 1 and 2 by a higher risk of hypoglycemia and a reduced incidence of ketoacidosis due to worsening glucagon secretion [62] and concomitant liver dysfunction in individuals with alcohol-related CP [2]. Complications such as macro-/microangiopathy, nephropathy, neuropathy and retinopathy are as common as in type 1 diabetes [62]. They largely depend on the duration of the disease, rarely affecting life expectancy, since the determining factors of prognosis for patients with CP are the outcomes of alcohol and nicotine addiction (cardiovascular diseases, malignant tumors).
Diagnosis of endocrine insufficiency should be timely and thorough, based on the results of regular determination of the concentration of glycosylated hemoglobin (HbA1c), fasting blood glucose level or glucose loading test. The optimal form of screening remains controversial [2]. An international expert committee with members nominated by the American Diabetes Association, the European Association for the Study of Diabetes Mellitus, and the International Diabetes Federation recommended using HbA1c (at a level ≥ 6.5) rather than blood glucose concentration to diagnose diabetes [63]. The advantages of HbA1c include the lack of a strict fasting determination and the lower variability of blood glucose results [2].
The diet for pancreatogenic diabetes corresponds to that for type 1 diabetes, with the exception of the need to correct malabsorption, deficiency of vitamins and microelements, and prevent hypoglycemia using fractional nutrition [1]. Most patients with secondary diabetes and ineffective diet require insulin. With the development of diabetes, oral hypoglycemic agents do not play a significant role in the outcome of severe fibrosis of the pancreatic parenchyma [64].
When prescribing insulin therapy, the target glucose level should correspond to that for type 1 diabetes, with the exception of a slight increase during episodes of severe hypoglycemia. To prevent severe hypoglycemia, patients are advised to stop drinking alcohol, increase physical activity, and eat smaller meals. Commitment to the TFT is of great importance. Patients on insulin therapy should avoid hypoglycemia.