Monocytes are one of the types of white blood cells. Their functionality is of great importance for ensuring and maintaining the health of the human body.
They perform such important functions as antitumor, antiviral and others. However, often after taking blood tests you can hear from the doctor that the level of monocytes is increased. Unfortunately, few people know what this statement means and how to correct the situation.
And, most importantly, does such a phenomenon pose any danger in the body.
What are monocytes, the mechanism of their formation
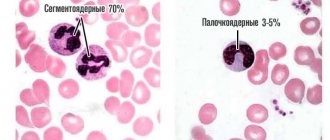
Monocytes are white blood cells with a diameter of 18 to 20 microns, belonging to agranulocytic leukocytes. These are the largest cells in the peripheral bloodstream. Microscopically, a monocyte is defined as an oval cell with one polymorphic nucleus, shaped like a bean. The core is in an eccentric position. The pronounced coloring of the monocyte nucleus distinguishes it from lymphocytes. When assessing a blood test, this sign allows you to correctly assess the blood picture. Healthy indicators of monocytes are 3-11% of the total volume of white blood cells.
A significant number of these cells are determined in:
- spleen;
- liver;
- lymph nodes;
- bone marrow.
The formation, development and growth of monocytes proceeds to the bone marrow under the influence of active substances:
- Glucocorticosteroids that can slow down the synthesis of monocytes.
- Cell growth factors GM-CSF and M-CSF, which stimulate the development of monocytes.
Formed mature monocytes function in the bloodstream for 2-3 days. Some of them die during this period due to physiological apoptosis, which is provided for by normal natural processes in the body. The remaining cells transform into macrophages and spread throughout internal organs and tissues. The life cycle of these advanced cells is 1 to 2 months.
Special qualities of monocytes
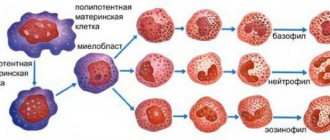
The bulk of monocytes are synthesized in the bone marrow. The first to emerge from a multipotent stem cell is a monoblast. Subsequently, it goes through the promyelomonocyte phase, and then the promonocyte phase. Promonocytes in the last stage of maturation have a pale, loose nucleus; traces of nucleoli are visible in the cytoplasm. Azurophilic granules are detected in mature monocytes and promonocytes. Both types of cells belong to the agranulocytic type. Granules of immature cells, histogenic particles and lymphocytes are the result of protein discolloidosis of the cytoplasm and are stained with azure using the Romanovsky-Giemsa method. In the connective tissue of internal organs and lymph nodes, a small part of monocytes is formed.
Biologically active substances and hydrolytic enzymes were found in the cytoplasm of mature monocytes:
- Lipase.
- Protease.
- Verdoperoxidase.
- Carbohydrase.
Lactoferrin and myeloperoxidase are found in minimal quantities.
The human body is able to activate the synthesis of monocytes in the bone marrow slightly. The division of phagocytic mononuclear cells outside the bone marrow occurs extremely slowly and is limited. The mechanism for replacing dead specific cells is possible only with the help of monocytes spreading through the bloodstream. In peripheral blood, monocytes function for about 72 hours, after which they penetrate into the tissues of nearby organs. Here the process of their transformation into mature histocytes, highly differentiated macrophages - Kupffer cells of the liver, alveolar cells of the lungs and other organs is completed.
Non-professional phagocytes:
This group of cells includes several other types of phagocytes, which do not have a directed effect against specific “enemies”, since they do not know how to present antigens. They have phagocytic activity, but it is less pronounced than the other cells described above. Examples include skin cells, some elements of connective tissue, etc. There are animals whose retina and even eggs are capable of phagocytosis!
So, in the tissues and blood of the body there is a large
number of phagocyte cells. They interact with each other in a complex manner, and in some cases their correct interaction may be disrupted, which will lead to health problems.
Knowing the fragility of this system, it is important to prevent imbalances in it. To do this, you need to monitor your general condition, lead a correct lifestyle, be sure to immediately and completely treat all emerging diseases, and also take special means to support the immune system.
Transfer Factor drug
in this case, it is optimal: it has a unique immunomodulatory effect. The information molecules contained in it carry a huge baggage of immunological memory accumulated by many generations of living beings. The value of this information is increased by the fact that it is presented in a “language” familiar to our immune system, since it was obtained during the activity of the same phagocyte cells.
Information molecules transmit the available data to immune cells, which distribute it among themselves. This becomes an impetus for the normalization of organ function and the body’s natural self-healing, which is the key to strengthening and maintaining overall health.
Differences between macrophages and monocytes
Until the 70s of the 20th century, scientists were convinced that all monocytes eventually transform into macrophages. Any additional sources of the appearance of “cleaners” have not been identified. And only in 2008, after a series of studies, it was established that macrophages have different origins. Some of them are transformed from monocytes, the rest develop from precursor cells of various types during intrauterine development of the fetus.
The transformation of one cell into another goes through certain stages. After monocytes enter the internal tissues from the blood, their active growth begins. At the same time, the development of mitochondria and lysosomes occurs. Thanks to these internal rearrangements, monocyte macrophages acquire specific properties.
Dendritic cells:
Perhaps some readers are seeing such a name for the first time and previously did not even suspect that such cells even exist. Nevertheless, they exist, and are located in large quantities in human tissues. As a rule, they are located close to the external environment and organ cavities: under the gastric mucosa, in the alveolar tissue of the lungs, in the nasal mucosa, etc. They were called dendritic because their numerous long processes give them a branching structure and make them look like trees (dendron - tree).
In these tissues, cells mature, after which they are sent to areas of accumulation of lymphoid tissue, interact with lymphocytes and macrophages and increase their activity.
Biological role in the body
The biological role of monocytes is very diverse. The largest phagocytes are necessary for many functions:
- Phagocytosis.
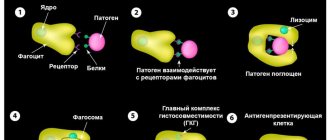
During this process, monocytes and macrophages identify proteins, bacteria, and viruses that are dangerous to the body, capture them and absorb them (phagocytose).
- Participation in the development of specific immunity.
Monocytes produce special cytotoxins, interferon, to counteract pathogenic viruses, bacteria and fungi.
- Assistance in the formation of allergic reactions.
Thanks to monocytes, specific elements of the compliment system are produced. Due to these processes, foreign proteins - allergens - are identified.
- Protection against tumors.
It is carried out through the production of tumor necrosis factor.
- Regulation of hematopoiesis and blood clotting processes
- carried out through the synthesis of specific elements.
Monocytes have special characteristics that distinguish them from neutrophils and other phagocytes:
- After absorbing a foreign element, monocytes do not die, but continue to function actively. In rare cases, the pathogen can defeat them.
- The life cycle of monocytes is longer than that of neutrophils.
- Monocytes have a pronounced antiviral effect, neutrophils have an antibacterial effect.
- When many monocytes are activated against a foreign agent, pus does not form.
- Chronic inflammatory process is a favorite place for concentration of macrophages and monocytes
Neutrophils:
These phagocyte cells are present in human blood, like monocytes, and there are a lot of them there. Neutrophils account for the majority of all leukocytes (50-75%). Throughout their five-day life, neutrophils protect our health. As soon as they receive a signal that there is a foreign object in some part of the body, they immediately leave the blood and within half an hour (!) approach the “scene of the disaster” to recognize and absorb the “offender.” The task of neutrophils, like macrophages, is self-sacrifice: having completed their task, they turn into pus cells.
The norm of monocytes in the blood
The rate of monocytes in peripheral blood ranges from 3 to 11%, which in absolute values is 0.04-0.08*109/liter. According to generally accepted medical decoding, monocytes are designated MON. Depending on the age of the person, their norm changes. Normal values are not determined by the gender of the patient.
| Person's age | Norm of MON parameters |
| from 1 to 15 days | 5%-15% |
| from 15 days to 1 year | 4%-10% |
| from 1 to 2 years | 3%-10% |
| from 2 to 15 years | 3%-9% |
| over 15 years old | 3%-11% |
A physiological increase in monocytes can be observed in women during pregnancy, but they do not go beyond normal limits.
The absolute volume of monocytes in one liter of blood is of great importance. These indicators differ for children and adults:
- Children under 12 years old - from 0.05 to 1.1 * 109 / liter.
- Over 12 years old - from 0.04 to 0.08*109/liter.
Reasons for the increase in monocytes in the blood
A detected increase in the level of monocytes above the established age norm is defined as monocytosis.
There are two types of this condition:
- Absolute monocytosis
characterized by an isolated increase in monocytes. Their level increases in adults by more than 0.8*109/l, for children under 12 years of age - more than 1.1*109/l. This symptom progresses against the background of certain pathologies in which the production of special phagocytes is activated.
- Relative monocytosis
characterized by a normal absolute value of monocytes, but an increase in their percentage in the blood. This occurs with a combined drop in the concentration of other leukocytes.
The state of absolute monocytosis raises alarming concerns among doctors, as it indicates a pathological process. Relative monocytosis is a temporary phenomenon and goes away on its own. In any case, an increase in the concentration of monocytes indicates that the body is resisting foreign elements.
Physiological causes of monocytosis
An increase in the monocyte index is observed in the first two hours after eating. This is a normal process for all people. Doctors insist that a general blood test be taken in the morning on an empty stomach, precisely for this reason.
An increase in monocytes in women is recorded in special physiological conditions:
- Menstruation.
At the beginning of the cycle, active rejection of endometrial cells occurs. In response to this, blood monocytes and macrophages rush to the site to perform their main function - cleansing. The highest concentration of monocytes is recorded during the period of heaviest bleeding. Independent normalization of phagocytes occurs after the end of bleeding. To get a more accurate picture, you should not take blood for a general analysis during menstruation.
- Pregnancy.
In the first three months of pregnancy, an active transformation of a woman’s immunity begins. Due to all the changes, there is a temporary decrease in the level of monocytes. Gradually their concentration changes and reaches a maximum in the third trimester, especially before childbirth. It should be noted that the peak values do not exceed the limits of normal values for the corresponding age.
When a general blood test reveals an increase in monocytes above normal levels, the state of monocytosis is defined as pathological. In such cases, professional medical assistance is necessary.
Infectious diseases
An increase in phagocytes occurs during infectious diseases. For example, in acute respiratory viral infections, the values of monocytes in a general blood test exceed the age limits several times. During the action of bacterial pathogens, there is an increase in neutrophils, and during viral pathogens, monocytes are used. The activity of phagocytes persists throughout the illness and for 2-4 weeks after recovery.
The persistence of monocytosis for 6-8 weeks or longer indicates a chronic course of the infectious disease. A slight excess of the upper norm is observed during colds - up to 0.09-1.5*109/l. A pronounced increase in monocytes up to 30-50*109/l may indicate the development of oncohematological diseases.
In pediatrics, monocytosis most often becomes a companion to infectious diseases.
Infectious mononucleosis
A common disease caused by the herpes-like Epstein-Barr virus. For adults, the infection is not dangerous due to the developed immune system.
The clinical picture progresses sharply and is characterized by the following manifestations:
- Fever up to 38-40 °C is characterized by a long course with periods of improvement and exacerbation. Features of temperature are the property that distinguishes the disease from ARVI.
- Rhinitis, sore throat.
- Hypertrophy of the lymph nodes in the occipital and submandibular region without pain.
- Skin rashes.
- Expansion of the boundaries of the spleen and liver.
- In the CBC there is an increased level of monocytes and lymphocytes.
To clarify the diagnosis, it is possible to perform an analysis for the presence of specific antibodies. During treatment, targeted antiviral drugs are not prescribed. Symptomatic therapy is carried out.
Childhood infections
Most childhood infections are transmitted by humans once and do not occur after adulthood. They are characterized by increased levels of monocytes and lymphocytes. This phenomenon is observed with a prolonged course of rubella, measles, whooping cough, and mumps.
Monocytosis in adults may be a reaction to the progression of more severe infectious diseases:
- Tuberculosis.
- Cytomegalovirus infection.
- Brucellosis.
- Syphilis.
- Typhoid fever.
- Sarcoidosis.
Helminthiasis
When parasites enter the body, they receive a quick response from the circulatory system. Monocytes are the first to react and begin to fight opisthorchiasis, roundworms, pinworms, bovine or pork tapeworms. Parasites familiar to our latitudes and exotic ones primarily affect the intestines.
Infestations manifest themselves in the form of specific symptoms:
- Sharp pain in various parts of the abdomen.
- Dyspeptic breakdown like diarrhea.
- Loss of body weight while maintaining or increasing appetite.
- Skin allergy in the form of urticaria.
In the blood, along with monocytosis, an increase in the level of granulocytic leukocytes - eosinophils, which regulate the formation of an allergic response, is recorded. To determine the type of parasite, stool is taken from the patient, bacterial cultures and immunological tests are performed. Therapy is specific and consists of taking antiparasitic drugs.
Chronic infectious and inflammatory diseases
Prolonged infection with unexpressed symptoms weakens the body, causing an increase in monocytes in the blood and the concentration of macrophages in the internal organs. The development of the clinical picture is influenced by the localization of the infectious process and the type of pathogen.
Monocytosis can be a symptom of an infection of the throat, lungs, bones, bacterial effects on the myocardium, kidneys, pelvic organs, and gall bladder. The course of chronic diseases is accompanied by periodic or constant pain in the affected area. An increase in temperature does not always appear. The success of adequate treatment depends on prompt identification of the cause. Therapeutic measures help relieve symptoms and restore the physiological level of monocytes in the blood.
Autoimmune disorders
Under the influence of certain factors, the immune system can become distorted. These disorders cause immune cells to identify their own elements as foreign and attack them. In autoimmune diseases, macrophages and monocytes rush to joints, kidneys, skin, and cardiac tissues, which appear as suspicious lesions.
The most common autoimmune disorders include:
- Diffuse toxic goiter, the main symptom of which is the active synthesis of thyroid hormones.
- Rheumatoid arthritis causes joint damage.
- Systemic lupus erythematosus is a serious disease that affects the tissues of internal organs, joints, and skin.
- Systemic scleroderma primarily affects the skin and then spreads to internal tissues.
- Diabetes mellitus (insulin-dependent type) causes a disorder in glucose metabolism and subsequent metabolic disorders throughout the body.
The detection of monocytosis in a blood test is not a clear symptom of an autoimmune disease. If the reasons for the shift in blood composition are not clear, additional diagnostic measures should be performed.
Oncohematological diseases
Malignant changes in the hematopoietic system are always accompanied by pronounced monocytosis. For their treatment, serious protocols are used, which are not always effective. After fixing an excessive level of monocytes, the patient should exclude autoimmune and infectious diseases. If the reasons for the changes cannot be established, there is a need to consult an oncohematologist.
Monocytosis can be a manifestation of serious diseases of the hematopoietic system:
- Acute leukemia of monocytic or myelomonocytic type.
With this pathology, monocyte precursors are determined in blood and bone marrow tests. The majority of patients are children under two years of age. Symptoms: anemia, bleeding, frequent infectious diseases, pain in bones and joints. The disease is characterized by an unfavorable course.
- Multiple
myeloma.
The main patients are people over 60 years of age. Symptoms: bone pain, frequent fractures, bleeding, decreased protective properties of the body.
Oncohematological disorders lead to a fairly high content of monocytes in the blood - more than 30-50*109/l. Indicators of this level give reason to believe that monocytosis is caused not by infectious factors, but by a malignant process. In the case of chronic inflammation, monocytes increase slightly, and in myeloma and leukemia, the number of agarnulocytes suddenly reaches high values.
Other cancers
Hodgkin's disease is one of the pathologies that should be excluded in case of monocytosis. Lymphogranulomatosis can manifest itself in the form of focal signs of internal organs, high fever, and hypertrophy of the lymph nodes. Symptoms of spinal cord damage may appear. In order to make a correct diagnosis, a biopsy of the lymph nodes is performed for histological analysis of the contents.
Monocytosis can be detected in the blood in various types of tumors. Detailed diagnostics using hardware research methods helps determine the nature and localization of the malignant process.
Intoxication with chemical reagents
Monocytosis can occur under specific conditions:
- Tetrachloroethane poisoning.
A toxic substance can enter the body through the upper respiratory tract, orally or by contact. Signs of intoxication: headache, yellowness of the skin, irritation of the mucous membranes. In severe cases, it causes liver failure and coma.
- Phosphorus poisoning.
Intoxication occurs when a toxic substance is ingested orally or by air. Symptoms: severe abdominal pain, diarrhea, nausea. The lack of adequate therapy leads to irreversible changes in the kidneys, liver, and central nervous system.
In case of poisoning, not only monocytosis is recorded, but also other pathological abnormalities in laboratory tests.
Read more: Monocytes are elevated: what does this mean? What to do?
Diagnostic value of simultaneous increase in other types of leukocytes
To make a diagnosis in a blood test, it is important to detect not only elevated monocytes, but also other cells of the leukocyte series. Together they:
- indicate the stage of the disease;
- determine the prognosis;
- confirm the type of infectious agent;
- determine the degree of loss of immunity.
Let's look at the most common reactions of blood cells.
Monocytes + lymphocytes
When monocytes and lymphocytes are elevated, an acute viral infection should be suspected: influenza, respiratory disease, measles, rubella, chickenpox. Against this background, a decrease in neutrophils is observed.
It is clear to the doctor that it is necessary to prescribe antiviral drugs.
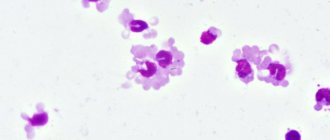
This is what different types of leukocytes look like under a microscope
Monocytes + eosinophils
For elevated monocytes and eosinophils, the necessary conditions are usually allergic reactions and parasitic infection (chlamydia and mycoplasma).
A distinctive symptom in patients is a long, painful dry cough in the absence of wheezing in the lungs and other clinical manifestations.
Monocytes + basophils
Basophils are fast-reacting cells; they manage to approach the source of infection while others are still “considering the information received.” If monocytes and basophils increase, it is necessary to exclude the influence of long-term treatment with hormonal agents.
The growth of basophils always accompanies an increase in macrophages and lymphocytes. They act by producing serotonin, histamine and other substances that increase inflammation.
Reasons for the decrease in monocytes in the blood
A decrease in monocyte levels in the blood below the appropriate age norm is called monocytopenia.
The cause of such changes in the composition of the blood may be certain conditions:
- Aplastic anemia.
- Purulent infections of bacterial origin.
- Late stages of oncohematological pathologies.
- Long-term use of medications.
Purulent bacterial infections
With purulent diseases caused by streptococcus or staphylococcus, the body becomes infected and an inflammatory process develops.
Among the infections that cause such changes, the following should be highlighted:
- Skin diseases - furunculosis, phlegmon, carbuncle.
- Osteomyelitis is a purulent bone lesion.
- Bacterial pneumonia.
- Sepsis is a severe blood infection characterized by a worsening of the patient’s general condition.
Aplastic anemia
A disease of the hematopoietic system that occurs as a result of inhibition or arrest of the growth and maturation of monocytes, red blood cells, leukocytes and platelets in the bone marrow. Symptoms: general weakness, decreased performance, dizziness, increased heart rate, constant pallor of the skin, bleeding, frequent infectious diseases, weakening of the body's protective properties.
In the absence of specific therapy, aplastic anemia leads to the death of the patient. This serious disease is treated by using cytostatics, hormonal drugs, and in severe cases a bone marrow transplant is required.
Oncohematological pathologies
Severe, long-term course of leukemia causes suppression of hematopoietic processes. Against this background, pancytopenia develops - a deficiency of all blood cells, including monocytes. The patient may experience severe infections due to immune disorders. Bleeding of unknown etiology often develops. Only timely bone marrow transplantation can stop the deterioration of the situation and promote the patient’s recovery.
Treatment with certain drugs
Long-term use of cytostatics and corticosteroids can lead to a deterioration in the hematopoietic activity of the bone marrow. This manifests itself in negative changes in blood composition. If a reduced content of certain blood cells is detected, the drug is discontinued and appropriate treatment is carried out. Timely measures help restore the normal state of the bone marrow.
Read more: Monocytes are low: what does this mean? How to increase?
Causes of monocytosis
The causes of monocytosis with a pathological increase usually reflect the degree of participation of one’s own immunity in anti-inflammatory activity. Elevated monocytes in the blood are detected when:
- viral infections (flu, respiratory disease, mumps, mononucleosis);
- bacterial and fungal infections (tuberculosis, syphilis, candidiasis);
- helminthic infestation in children;
- rheumatic damage to the heart and joints;
- bacterial septic endocarditis;
- enteritis, colitis of bacterial and fungal etiology;
- cases of sepsis;
- conditions after surgical treatment of appendicitis, gynecological operations;
- systemic autoimmune diseases (rheumatoid polyarthritis, sarcoidosis, lupus erythematosus);
- tumors from the blood line (lymphogranulomatosis, myeloid leukemia, thrombocytopenic purpura);
- malignant tumors.