Prohibited during pregnancy
Prohibited during breastfeeding
Prohibited for children
Allowed for older people
Has limitations for liver problems
Allowed for kidney problems
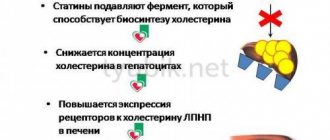
Today, the danger of increased concentrations of bad cholesterol in blood plasma has been proven. Hypercholesterolemia can cause serious pathologies, which quite often lead to death. Statins are the most effective medications for lowering cholesterol levels in the blood. This effectiveness is based on their mechanism of action on the body.
There are a large number of statins, but recently drugs of the latest generations are increasingly being prescribed - 3rd generation (Atorvastatin) and 4th generation (Rosuvastatin). These drugs act approximately the same way, but with slight differences, so it is worth finding out which is better - Rosuvastatin or Atorvastatin in each specific case.
Review of Atorvastatin and Rosuvastatin
Atorvastatin is a drug that has a hypocholesterolemic effect.
As it passes through the body, the inhibitor controls the functionality of enzyme molecules that regulate the synthesis of mevalonic acid. Mevalonate is a precursor to sterols, which are found in low-density lipoproteins. 3rd generation statin tablets are used in the treatment of high cholesterol. During the period of atherosclerotic manifestations, the use of the drug shows a positive effect on lipid metabolism, reducing the concentration of lipid fractions of LDL, VLDL and triglycerides, which are the basis for the formation of atherosclerotic tumors. When using the drug, the cholesterol index decreases, regardless of its etiology.
Properties of statins
The drug Rosuvastatin is prescribed when there is an increased concentration of LDL molecules in the blood plasma. The drug belongs to the group of fourth (last) generation statins, where the main active ingredient is rosuvastatin. The latest generation medications containing rosuvastatin are the safest for the body and also have a high therapeutic effect in the treatment of hypercholesterolemia.
What are statins?
Statins are a separate category of lipid-lowering (lipid-lowering) drugs used to treat hypercholesterolemia, i.e. persistently elevated levels of cholesterol (XC, Chol) in the blood, which cannot be reduced using non-drug methods: a healthy lifestyle, sports and diet.
In addition to the main effect, statins have other beneficial properties that prevent the development of severe cardiovascular complications:
- maintaining the growth of atherosclerotic plaques in a stable state;
- blood thinning by reducing platelet and red blood cell aggregation;
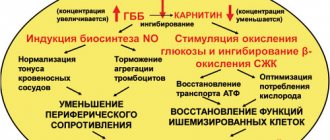
- relief of endothelial inflammation and restoration of its functionality;
- stimulating the synthesis of nitric oxide, necessary for vascular relaxation.
Typically, statins are taken when the permissible cholesterol level is significantly exceeded - from 6.5 mmol/l, however, if the patient has aggravating factors (genetic forms of dyslipidemia, existing atherosclerosis, heart attack or stroke in history), then they are prescribed at lower levels - from 5 .8 mmol/l.
Composition and principle of action
The composition of the drugs Atorvastatin and Rosuvastatin includes synthetic substances from the latest generations of statins in the form of calcium salt - atorvastatin calcium (III generation) and rosuvastatin calcium (IV generation) + auxiliary components, including dairy derivatives (lactose monohydrate ).
The action of statins is based on inhibition of the enzyme responsible for the production of cholesterol by the liver (the source of about 80% of the substance).
The mechanism of action of both drugs is aimed at inhibiting the key enzyme responsible for the production of cholesterol: by suppressing (inhibiting) the synthesis of HMG-CoA reductase in the liver, they reduce the production of mevalonic acid, a precursor of internal (endogenous) cholesterol.
In addition, statins stimulate the formation of receptors responsible for the transport of low-density lipoproteins (LDL), especially low-density lipoproteins (VLDL, VLDL) and triglycerides (TG) back to the liver for disposal, which leads to a sharp decrease in “bad” cholesterol fractions in blood serum.
A feature of new generations of statins is also that they do not affect carbohydrate metabolism, i.e. Atorvastatin and Rosuvastatin only slightly increase the concentration of glucose, which allows them to be taken even by people with a non-insulin-dependent form of type II diabetes mellitus.
The principle of action of the drugs
Atorvastatin is a lipophilic drug that is soluble only in fats, and Rosuvastatin is a hydrophilic drug that is highly soluble in plasma and serum.
The effect of modern drugs is so effective that for many patients one course of drug treatment is enough to reduce total cholesterol, LDL and VLDL fractions, as well as triglycerides.
Mechanism of action of statins
Both drugs are inhibitors of HMG-CoA reductase molecules. Reductase is responsible for the synthesis of mevalonic acid, which is part of sterols and is part of the cholesterol molecule. Cholesterol molecules and triglycerides are components of very low molecular density lipoproteins, which are combined during synthesis in liver cells.
With the help of the drug, the amount of cholesterol produced is reduced, which triggers LDL receptors, which, when activated, begin hunting for low-density lipids, capturing them and transporting them for disposal.
Thanks to this work of receptors, there is a significant decrease in low-density cholesterol and an increase in the content of high-density lipids in the blood, which prevent the development of systemic pathologies.
For comparison, Rosuvastatin does not require transformations in liver cells to begin acting, and it begins to act faster, but this medication does not affect the reduction of triglycerides. Unlike the latest generation of medications, Atorvastatin is converted in the liver, but it is also effective in lowering the TG index and free cholesterol molecules due to its lipophilicity.
Reviews
Oksana, 46 years old, Pyatigorsk: I took Atorvastatin to lower cholesterol. It reduces well, but I experienced side effects myself. After 3 months of regular use, almost all lipid profile indicators, except triglycerides, approached normal. Based on the results of the analysis, the doctor supplemented the treatment with Dibikor, and triglycerides also decreased. I was afraid for my liver, but in vain. Everything is fine there.
Ekaterina, 35 years old, Moscow: I can’t say that Atorvastatin is significantly different in effectiveness from previous drugs. My father was prescribed 60 mg per day; he has high cholesterol. He says that he does not notice any significant changes in his condition after the course of treatment. Cholesterol remains what it was. Apparently this is due to hereditary predisposition.
Kirill, 60 years old, Samara: With a diagnosis of coronary heart disease, the doctor prescribed statins to prevent complications. The choice fell on the drug Rosuvastatin. I don’t feel its influence on myself, but according to tests, cholesterol corresponds to the norm for a healthy person. Before starting to take Rosuvastatin, it was increased several times. I can confidently recommend this drug to others to reduce high cholesterol.
Indications and contraindications
Both drugs have the same direction in the treatment of high cholesterol, and, despite the differences in chemical structure, both are HMG-CoA reductase inhibitors. Statin tablets should be taken for the following lipid imbalances:
- hypercholesterolemia of various etiologies (family hereditary and mixed);
- hypertriglyceridemia;
- dyslipidemia;
- systemic atherosclerosis.
Dyslipidemia
Medications are also prescribed to patients at high risk of developing vascular and cardiac pathologies:
- hypertension;
- angina pectoris;
- cardiac ischemia;
- ischemic and hemorrhagic stroke;
- myocardial infarction.
The cause of hypercholesterolemia is a disorder in lipid metabolism, which often occurs through the fault of the patient himself due to an incorrect lifestyle.
Taking statins will help prevent the development of pathology if taken regularly for preventive purposes in the presence of the following factors:
- food with a high content of animal fat in products;
- alcohol and nicotine addiction;
- nervous tension and frequent stress;
- not an active lifestyle.
The contraindications for these two medications are different (Table 2).
| Rosuvastatin | Atorvastatin |
|
|
Features of Rosuvastatin
Rosuvastatin is a lipid-lowering agent and is prescribed to normalize the level of triglycerides and phospholipids and lipoproteins in the blood. The main active ingredient is rosuvastatin. It is prescribed for the treatment and prevention of hypercholesterolemia, atherosclerosis and its complications, and vein thrombosis.
Rosuvastatin reduces high concentrations of low-density cholesterol, total cholesterol, triglycerides, and apoliprotein. At the same time, it helps to increase the level of high-density lipoproteins. While taking this drug, the atherogenicity index decreases. This effect indicates normalization of the lipid profile.
Indications for prescribing this drug are as follows:
- hereditary tendency to increase cholesterol;
- initial detection of high cholesterol levels in the blood;
- increased levels of triglycerides in the blood;
- prevention of complications of atherosclerosis, namely angina pectoris, hypertension, myocardial infarction and stroke in patients over 50 years of age.
Since Rosuvastatin is not metabolized in the liver, its effect on this organ is minimal. After 90% of the drug is excreted through the intestines with feces, the rest through the kidneys with urine. The drug is not prescribed to persons under 18 years of age, patients with lactose intolerance, women during pregnancy and breastfeeding.
It is contraindicated in patients at the acute stage of liver disease, patients with myopathy, and those with individual intolerance to the components of the drug. The combination of Rosuvastatin with Cyclosporine is unacceptable. During treatment with this statin, doctors recommend following an anti-cholesterol diet. When prescribing a drug in a dosage of more than 40 mg, the attending physician takes into account the absolute and relative indications for this.
Rosuvastatin lowers cholesterol levels better than all other similar drugs
Both drugs - Atorvastatin and Rosuvastatin - have good patient reviews. Since these medications have similar effects, they are interchangeable. But the choice of a particular one should be determined by the doctor in accordance with the diagnosis and individual characteristics.
Instructions for use
Statins should be taken orally with a sufficient amount of water. It is forbidden to chew the tablet because it is coated, which dissolves in the intestines. Before starting a therapeutic course of 3rd and 4th generation statins, the patient must adhere to an anti-cholesterol diet, and the diet must accompany the entire course of medication treatment.
The doctor individually selects the dosage and drug for each patient, based on the results of laboratory tests, as well as the individual tolerance of the body and concomitant chronic diseases. Dose adjustments, as well as replacement of the drug with another medicine, are carried out no earlier than two weeks from the date of administration.
Atorvastatin dosage regimens
The initial dosage for systemic atherosclerosis is Rosuvastatin - 5 mg, Atorvastatin - 10 mg. You need to take the medicine once a day.
Daily dosage for the treatment of hypercholesterolemia of various etiologies:
- for homozygous hypercholesterolemia, the dosage of Rosuvastatin is 20 mg, Atorvastatin is 40-80 mg;
- in patients with heterozygous hypercholesterolemia - 10-20 mg of Atorvastatin, divided into morning and evening doses.
Can Atorvastatin be replaced with Rosuvastatin?
In case of poor tolerability of the drug, which is expressed by negative consequences for the liver, confirmed by deterioration of laboratory parameters, it is necessary to adjust the Atorvastatin dosage regimen: temporarily discontinue it, reduce the dosage, or you can replace it with the newest Rosuvastatin.
You cannot do this on your own, because usually 2–4 weeks after stopping the medication, the level of lipids in the blood returns to its original value, which can greatly worsen the patient’s health. Therefore, the decision about the possibility of replacement should be made together with your doctor.
Key differences and effectiveness
What is the difference between Rosuvastatin and Atorvastatin? The difference between medications is obvious at the stage of their absorption from the small intestine. Rosuvastatin does not need to be tied to the time of food intake, and Atorvastatin begins to lose its properties if you take the tablet during dinner or immediately after it.
This medication is also affected by taking other medications, because its conversion into an inactive form occurs with the help of liver cell enzymes. The drug is removed from the body along with bile acids.
Additional effects of statins
Rosuvastatin is excreted unchanged in the feces. Do not forget that any long-term treatment requires financial resources. Atorvastatin costs 3 times less than a 4th generation statin, so it is available to different segments of the population. Price for Atorvastatin (10 mg) – 125 rubles, 20 mg – 150 rubles. The cost of Rosuvastatin (10 mg) is 360 rubles, 20 mg – 485 rubles.
Each drug will work differently in each patient's body. The doctor selects medications in accordance with age, pathology, stage of its progression and lipid profile indicators. Atorvastatin or Rosuvastatin reduce bad cholesterol almost equally - within 50-54%.
The effectiveness of Rosuvastatin is slightly higher (within 10%), so these properties can be used when the patient’s cholesterol is reduced above 9-10 mmol/l. Also, this drug is able to reduce total cholesterol in a shorter period of time, which reduces the number of side effects.
Currently, in developed countries, up to 80–95% of patients with coronary heart disease (CHD) take statins. These figures indicate that cardiologists have no doubt about the advisability of such treatment. Indeed, in recent years, data from several very large studies have been published, which clearly indicate a decrease in mortality (both cardiovascular and general) during therapy with these drugs. In addition, many additional effects of statins have been described and can be used alone. This is, for example, a significant anti-ischemic effect observed with long-term use of these drugs. The anti-inflammatory effects of statins are so great that attempts are being made to treat rheumatoid arthritis with their help. There have been reports of the clinical effectiveness of statins in demyelinating diseases.
However, despite the widespread use of statins, target levels of lipids (primarily atherogenic fractions) are not always achieved. At the same time, a decrease in the incidence of complications of coronary atherosclerosis is associated with the correction of this particular risk factor. Attempts to combine statins with other lipid-lowering drugs are not always successful, as they can lead to the development of severe side effects (as was the case with cerivastatin, which in combination with fibrates led to the development of a large number of cases of rhabdomyolysis). There is evidence of the combined use of statins and nicotinic acid. However, nicotinic acid itself has a very wide range of side effects.
Currently, the use of maximum dosages of statins is actively recommended. However, this makes treatment so expensive that even in developed countries this approach is not widely used. Thus, monthly treatment with atorvastatin (the most popular statin in the United States) at a dose of 80 mg (excluding the cost of monitoring safety parameters) will cost almost $400. In our country, where such a dosage is not registered, taking 8 tablets (10 mg) of atorvastatin per day will cost the patient $400–500 monthly. But even such doses do not always lead to achieving the target level of low-density lipoproteins (LDL).
Comparison of moderate and aggressive lipid-lowering statins
During 2004, the results of 2 interesting studies were published comparing statins - pravastatin, which has a very moderate effect on LDL levels, and atorvastatin, which reduces LDL levels to a much greater extent. The data obtained indicate that the administration of statins, which intensively lower lipid levels, leads to a more pronounced clinical effect.
REVERSAL Study
This study (Reversal of Atherosclerosis with Aggressive Lipid Lowering) compared the effect of 40 mg of pravastatin and 80 mg of atorvastatin per day on the dynamics of atherosclerotic lesions of the coronary bed by changes in the volume of coronary atheroma [1]. Of the 2163 patients screened, 654 patients were randomized and received study drugs. Of these, 502 patients were able to perform intravascular ultrasound of satisfactory quality at baseline and after 18 months of therapy, with 249 patients included in the pravastatin group, 253 in the atorvastatin group. The baseline LDL level in both groups was 150.2 mg/dL (3.89 mmol/L). During treatment with pravastatin, the content of this fraction decreased to 110 mg/dl (2.85 mmol/l), and when using atorvastatin - to 79 mg/dl (2.09 mmol/l). According to this indicator, the differences turned out to be highly significant (p
The studied statins had different effects on atheroma volume. If atherosclerotic lesions progressed during treatment with pravastatin (increase by 2.7%, p = 0.001), then in the atorvastatin group its volume did not change.
PROVE-IT Study – TIMI-22
The Pravastatin or Atorvastatin Evaluation and Infection Therapy – Thrombolysis in Myocardial Infarction 22 (PROVE-IT – TIMI-22) study also compared the effects of atorvastatin (80 mg/day) and pravastatin (40 mg/day) [2].
4162 patients were randomized - men and women over 18 years of age who were hospitalized for acute coronary syndrome (with or without ST-segment elevation) or who had an episode of high-risk unstable angina within 10 days before inclusion in the study. Total cholesterol levels should not exceed 240 mg/dL (6.21 mmol/L) or 200 mg/dL (5.18 mmol/L) if patients had previously received statins. The study did not include patients who had previously received statins at a dose of 80 mg/day, or patients using drugs metabolized by the 3A4 isoenzyme of the cytochrome P450 system.
The pravastatin group included 2063 patients and the atorvastatin group - 2099. The groups were completely comparable in all main clinical characteristics, with the exception of the incidence of peripheral atherosclerosis, which was more often observed among patients receiving pravastatin (p = 0.03). The follow-up period ranged from 18 to 36 months (average 24 months). After 925 endpoints were recorded, the study was stopped.
Endpoints included death from any cause, myocardial infarction, documented unstable angina requiring hospitalization, revascularization (angioplasty or coronary artery bypass grafting) performed more than 30 days after randomization, and stroke.
A significant difference between the groups in LDL levels was noted already from the 30th day of treatment. When using pravastatin, its average concentration was 95 mg/dl (2.46 mmol/l), and in the atorvastatin group it was 62 mg/dl (1.60 mmol/l). In patients previously treated with statins, additional pravastatin did not reduce LDL levels, while atorvastatin reduced their concentration by another 32%. In patients who had not previously taken statins, LDL cholesterol levels decreased by 22% when treated with pravastatin, and by 51% when using atorvastatin. At the same time, the level of high-density lipoproteins (HDL) increased to a greater extent in the pravastatin group (8.1 vs. 6.5%, p
Differences in the degree of reduction in CRP levels also turned out to be highly significant. Although its content significantly decreased in both groups, with pravastatin its level decreased to 2.1 mg/l, and with atorvastatin - to 1.3 mg/l (initial level - 12.3 mg/l in both groups ).
The main result of the study was a 16% (p = 0.005) lower incidence of endpoints in the atorvastatin group. During 2 years of observation, the incidence of adverse outcomes with pravastatin was 26.3%, and only 22.4% with atorvastatin. The difference between the groups began to be noted on day 30 of treatment and persisted throughout the study.
During treatment with atorvastatin, the incidence of unstable angina requiring hospitalization (by 29%, p = 0.02) and the need for revascularization (by 14%, p = 0.04) were significantly lower. Reductions, although not significant, were also observed in the risk of death from any cause (by 28%, p = 0.07) and the combined endpoint of death + myocardial infarction (by 18%, p = 0.06). Stroke was rare in both groups, and there was no significant difference in this endpoint between the groups.
The benefit of atorvastatin was greatest in patients with baseline LDL levels greater than 125 mg/dL (34% risk reduction for the composite endpoint, p = 0.02) and in patients who had not previously received statins.
The importance of the results demonstrating a clear advantage of atorvastatin also lies in the fact that they were obtained in a study conducted by the company that produces pravastatin, whose specialists had reason to assume completely different results. The main hypothesis underlying the protocol was that there would be no difference in the clinical effects of the two statins, despite differences in lipid-lowering effects.
The concept is the lower the better”
In July 2004, amendments to message 3 of the US National Cholesterol Education Program were published in the journal Circulation [3]. Based on the results of recently published studies, it was decided to significantly tighten the requirements for blood LDL levels (Table 1).
It is proposed to identify 4 risk groups for the development of coronary death over the next 10 years. The high-risk group includes conditions that correspond to the risk of a heart attack or coronary death in more than 20% of cases over the next 10 years. This is a history of coronary artery disease (myocardial infarction, unstable angina, stable angina, revascularization procedures), signs of significant myocardial ischemia. In addition, this risk is caused by the presence of so-called CHD risk equivalents in the patient. This is clinically significant non-coronary atherosclerosis, diabetes mellitus, or a combination of conditions in which the risk exceeds 20%.
In this group of patients, LDL levels should be below 100 mg/dL (2.6 mmol/L). However, there is evidence that this goal may be to reduce LDL concentrations below 70 mg/dL (1.8 mmol/L), especially in patients at very high risk (acute coronary syndrome). If the LDL level in such patients is greater than or equal to 2.6 mmol/l, lipid-lowering therapy is required along with lifestyle changes. However, there is evidence that statin therapy is indicated for such patients even in cases where the initial LDL level is below 2.6 mmol/l. High triglyceride levels or low HDL levels are an indication for additional fibrates or niacin. Moreover, if the concentration of triglycerides is above 2.3 mmol/l, then one of the goals of therapy is to achieve the level of atherogenic fractions of cholesterol (cholesterol of all fractions except HDL) below 3.4 mmol/l (0.8 mmol/l above the target LDL level ).
The next gradation – high intermediate risk – involves a combination of 2 or more risk factors, in which the incidence of myocardial infarction or coronary death over the next 10 years is 10–20%. This risk is caused by a combination of smoking and an increase in blood pressure over 140/90 mm Hg. Art., low HDL level (
The risk based on these factors is calculated using special calculator programs (on the Internet, such a calculator is located at www.nhlbi.gov/guidelines/cholesterol).
Intermediate risk is a combination of 2 or more risk factors for which the 10-year risk calculated using a calculator does not exceed 10%.
When lipid-lowering drugs are used in high- and intermediate-risk groups, LDL levels should be reduced by at least 30–40%.
It is also important that all patients actively adjust their lifestyle (increase in physical activity); carried out therapy aimed at reducing excess body weight and treating metabolic syndrome, eliminating hypertriglyceridemia and increasing HDL levels if they decreased.
In the low-risk group (0–1 risk factor), the risk of CAD should not be calculated.
European recommendations for the prevention of cardiovascular diseases are based not on calculating the risk of complications of coronary atherosclerosis, but on taking into account the total risk of cardiovascular diseases, including stroke.
The place of the anti-inflammatory effect in the antiatherogenic action of statins
The large number of effects of statins that are not associated with a decrease in the level of atherogenic lipoproteins allows us to seriously discuss the question of what is more important - their effect on cholesterol synthesis or other consequences of blockade of mevalonic acid metabolism.
The anti-inflammatory effect of statins has received the most attention. The participation of inflammatory reactions in atherogenesis is now considered proven. It has been established that the prognosis for atherosclerotic lesions of various locations can be significantly clarified by measuring the level of inflammatory markers in the systemic circulation. Most often, this is done by determining the level of CRP using a highly sensitive technique. Based on data from large epidemiological studies, it is proposed to divide the CRP level into 3 ranges: low - less than 1.0 mg/l, medium - 1.0-3.0 mg/l and high - more than 3.0 mg/l. A CRP level above 10 mg/L indicates the presence of causes for a systemic inflammatory response, such as infection, trauma, etc. To assess the risk of atherosclerosis, this test should be repeated 2 weeks after the relief of these conditions.
CRP is a non-glycosylated protein, the main regulator of whose synthesis is interleukin 6. The stimulus that provokes the synthesis of CRP can be oxidized lipoproteins. Until recently, it was believed that CRP is synthesized by hepatocytes, but recently it has been discovered that it can also be produced in atherosclerotic plaques, kidneys, nervous tissue and alveolar macrophages. Recently, information has emerged that CRP is not only a marker of the inflammatory process in atherosclerosis, but is itself an active factor in atherothrombosis.
The effect of CRP on endothelial cells leads to a decrease in the activity of endothelial NO synthetase, a decrease in the synthesis of prostacyclin, an increase in the production of type 1 plasminogen activator inhibitor, endothelin-1, interleukins 6 and 8, and some cell adhesion molecules that provoke the migration of macrophages into the subendothelial layer. The proatherogenic effect of CRP on smooth muscle cells is manifested by the acceleration of their proliferation, increased expression of angiotensin type 1 receptors and an increase in the level of inducible NO synthetase. The latter synthesizes nitric oxide, which is spent mainly on the formation of a very aggressive radical - peroxynitrite. Macrophages under the influence of CRP more actively produce free radicals, cytokines (interleukins 1 and 6, tumor necrosis factor), tissue factor, etc. [4]. All this confirms the direct participation of CRP in the processes of atherogenesis. Therefore, reducing its level can be considered as one of the main goals of pathogenetic treatment of atherothrombosis.
To date, several studies have been published comparing the effects of different statin regimens on CRP levels. A randomized, placebo-controlled trial of 110 patients compared the effects of treatment with atorvastatin (10–80 mg, target LDL level less than 2.1 mmol/L) and lovastatin (5–10 mg, target LDL level less than 3.4 mmol/L). l). A significant decrease in CRP levels (from 2.6 to 1.7 mg/l, p = 0.002) was achieved only with intensive lipid-lowering therapy with atorvastatin. In other words, there is a parallel between the effects of statins on lipids and inflammatory markers.
Rosuvastatin is the most effective statin
Rosuvastatin (Crestor) is a completely synthetic drug of the statin group, approved for clinical use in 2003. Due to its obvious advantages, the demand for rosuvastatin turned out to be very high. This is evidenced by the fact that since registration it has already been prescribed to more than 2.5 million patients, despite the presence of 5 other statins on the pharmaceutical market.
The pharmacokinetic characteristics of rosuvastatin and other currently used statins are presented in table. 2. After a single dose of rosuvastatin, its maximum concentration in the blood is reached after approximately 5 hours. The drug has the longest half-life - 19 hours. This may be due to the phenomenon of enterohepatic recirculation demonstrated experimentally. Approximately 88% of rosuvastatin is reversibly bound to plasma proteins, mainly albumin.
The pharmacokinetic characteristics of rosuvastatin are not affected by age, gender, time of drug administration or concomitant food intake, as well as the presence of moderate liver failure.
The rosuvastatin molecule is hydrophilic, which makes it more selective towards hepatocytes than other tissues. Another consequence of the hydrophilicity of this drug is its significantly less effect on cholesterol synthesis in skeletal muscle myocytes. In studies conducted on cultured skeletal muscle cells, rosuvastatin and another hydrophilic statin, pravastatin, reduced the activity of cholesterol synthesis to a much lesser extent (50-1000 times) than the lipophilic atorvastatin, simvastatin and cerivastatin. This fact allows us to consider rosuvastatin potentially safer compared to other drugs from the statin group.
It has been shown that 90% of the drug is excreted in feces, and 10% in urine. Only 10% of rosuvastatin is metabolized; its main metabolite, N-desmethyl rosuvastatin, is approximately 2 times less active than the main substance. Unlike most statins (in particular, atorvastatin and simvastatin), rosuvastatin interacts minimally with enzymes of the cytochrome P450 system, and therefore the likelihood of its interaction with many widely prescribed drugs (antihistamines, antifungals, antiulcers, a number of antibiotics, antidepressants, cardiac glycosides, etc.) is minimal. In particular, the drug does not have an inhibitory effect on isoenzymes 1A2, 2C19, 2D6, 2E1 and 3A4. Only for the 2C9 isoenzyme, a decrease in its activity by 10% was noted. When rosuvastatin was co-administered with fluconazole (a potent inhibitor of the 2C9 isoenzyme), only a slight increase in statin concentrations was observed.
The clinical effectiveness of rosuvastatin is being actively studied in a series of studies, the program of which is called GALAXY (45 thousand participants). This program examines the effects of rosuvastatin on lipids, inflammatory markers, the dynamics of the atherosclerotic process and so-called fixed (or “hard”) endpoints. The program covers most of the conditions for which statins are currently used.
However, the greatest interest is in the AURORA study, which examined the effect of the drug in patients on hemodialysis; the CORONA trial, which included patients with heart failure, and the JUPITER trial, which focused on primary prevention in patients with normal LDL levels and elevated CRP levels. All these studies are ongoing and their results will resolve a number of unexplored issues.
Among those completed, the MERCURY I (Measuring Effective Reductions in Cholesterol Using Rosuvastatin therapy) study was of great importance for assessing the effectiveness of rosuvastatin. This open-label, randomized trial included 3161 patients with hyperlipidemia [5]. Its purpose was to compare the effectiveness of rosuvastatin, atorvastatin and other statins in terms of reducing LDL concentrations. The main criterion for assessing effectiveness was achieving the target LDL level. The study lasted 16 weeks.
The result of the study was the demonstration of a significant advantage of rosuvastatin over other statins in terms of their effect on lipids. The target LDL level while taking rosuvastatin at a dose of 10 mg/day was achieved in 86% of patients compared to 80% when using a similar dose of atorvastatin (p
Currently, rosuvastatin is recommended for use in dosages of 10–40 mg per day. At the same time, LDL levels are reduced by 52–63%, i.e. to a much greater extent than when using other statins in similar doses. In addition, treatment with rosuvastatin significantly increased the concentration of HDL by 14% and decreased the level of triglycerides by 28%.
Reducing the level of atherogenic fractions of cholesterol (primarily LDL cholesterol) is not the only goal of lipid-lowering therapy. It should also be aimed at correcting the content of HDL, a potentially antiatherogenic fraction of lipoproteins, the level of which is reduced in many patients.
At the last European Congress of Cardiology (2004), the results of the largest population-based study INTER-HEART were presented. It showed that 9 potentially modifiable factors determine the risk of myocardial infarction by 90%, with the most significant of them being the ApoB/ApoA1 ratio. In second place in importance is smoking, followed by diabetes mellitus, arterial hypertension, abdominal obesity, psychosocial factors, the amount of fruits and vegetables consumed, physical inactivity and alcohol consumption [6].
The fact that the most significant was the ratio of ApoB, the only protein included in LDL, to ApoA1, the HDL protein, once again confirms the special importance of maintaining this fraction of lipoproteins at an optimal level. The main competitor of rosuvastatin, atorvastatin, has a very slight effect on HDL concentrations. Moreover, as the dose of atorvastatin increases, the extent of its effect on HDL decreases.
Rosuvastatin behaves in the opposite way. The STELLAR study [7] showed that differences between it and atorvastatin in the effect on HDL appeared already when using these drugs at a dose of 10 mg, and when taking statins at a dose of 20 mg, the difference became highly significant. When using rosuvastatin at a dose of 10 mg, the level of ApoB decreased by 38%, and the concentration of ApoA1 increased by 5%. As a result, the ApoB/ApoA1 ratio decreased by 40%.
The pronounced hypotriglyceridemic effect of rosuvastatin can be considered proven in patients with initial triglyceride levels in the range from 3.4 to 9 mmol/l [8]. A randomized, placebo-controlled study that included 156 such patients showed that a 6-week course of rosuvastatin therapy leads to a decrease in triglyceride levels by 37–40%, and cholesterol of all atherogenic fractions by 42–51%. In parallel, HDL levels increase by 6–18%. This feature of the action of rosuvastatin allows us to expect that its widespread introduction into clinical practice will significantly reduce the need for the combined prescription of statins and fibrates.
Safety of rosuvastatin
The problem of treatment safety is the most important aspect of the use of any medicine. It becomes especially important when introducing into clinical practice a drug intended for a very large number of patients. Attention to the safe use of statins has increased sharply after the withdrawal of cerivastatin from the market, the uncontrolled use of which led to a large number of fatal complications.
The emergence of a new drug in this class, rosuvastatin, opened a discussion about the advisability of registering a new drug in conditions where a significant number of statins already exist and are actively used. That is why rosuvastatin has undergone very careful study from a safety point of view. Information for this drug was analyzed on twice the number of patients required for registration of other statins. One of the consequences of this test was some delay in the release of the drug to the market. On the other hand, its results allow us to confidently assert that, subject to dosages and rules for prescribing rosuvastatin, its use is at least as safe as other statins.
However, some precautions common to all statins must be taken when using rosuvastatin. Thus, in some patients, while using high doses of rosuvastatin, proteinuria may be observed, associated with the development of a kind of tubulopathy, which is also observed in 0.2–0.6% of cases when using other statins. Therefore, the drug should not be prescribed in a dose of 40 mg to patients with creatinine clearance less than 60 ml/min and in any dosage with creatinine clearance below 30 ml/min. In any case, when prescribing 40 mg of rosuvastatin, it is necessary to monitor the level of proteinuria.
Like other statins, rosuvastatin should be used cautiously in patients who abuse alcohol and have liver disease. All patients need to determine the level of liver transaminases initially and after 3 months of therapy. An increase in their level by more than 3 times is a reason to reduce the dose or discontinue the drug.
Pharmacokinetic studies have shown that patients belonging to the Mongoloid race are more sensitive to the effects of statins. Therefore, when prescribing rosuvastatin to such patients, slightly lower dosages should be used and the drug should not be used at a dose of 40 mg.
The most serious, although extremely rare, side effect of any statin is the development of rhabdomyolysis. Before starting the use of rosuvastatin, it is necessary to measure the initial level of creatine phosphokinase. If it increases more than 5 times after 5-7 days, the analysis must be repeated - if the increase persists, rosuvastatin therapy is not started. It was found that myopathy and rhabdomyolysis are more common in patients with kidney damage and hypothyroidism; in the presence of congenital muscle diseases in relatives; in patients who had signs of muscle tissue damage while taking other statins and fibrates; in persons who abuse alcohol; in cases where the drug is used in combination with fibrates. Such patients should not be prescribed rosuvastatin at a dose of 40 mg. The presence of myopathy is a contraindication to the use of the drug in all dosages.
Rosuvastatin is also contraindicated in women during pregnancy and lactation. It should not be prescribed to patients with preserved reproductive function if they do not use contraception.
In general, the safety profile of rosuvastatin does not differ from that of other statins. To date, its safety has been studied in more than 15 thousand patients, 1500 patients have taken the drug for more than 2 years. More than 45 thousand people are currently participating in controlled studies of rosuvastatin.
Thus, the feasibility of the widest use of statins in clinical practice does not raise any doubts today. In our country, as well as throughout the world, there are practically no doctors left who are unfamiliar with the therapeutic possibilities provided by drugs of this class. Unfortunately, statins are not always used correctly, in adequate dosages, which, of course, significantly reduces the effectiveness of their use as a means of preventing severe complications of atherosclerosis. A new representative of this class, rosuvastatin (Crestor), now available in Russia, surpasses all other statins in its ability to reduce the level of proatherogenic lipoproteins. Its most important advantages are also its beneficial effect on antiatherogenic fractions of lipoproteins (primarily HDL) and a powerful hypotriglyceridemic effect. This reduces the need for combined administration of statins and fibrates, which significantly increases the safety of lipid-lowering therapy. In addition, the effectiveness of the drug in most patients at an initial dose of 10 mg reduces the need for titration compared to other statins, increases adherence to treatment, and reduces the cost of therapy. Some features of the pharmacokinetics and pharmacodynamics of rosuvastatin allow us to expect better tolerability of this drug compared to other statins.
Adverse reactions
The negative effect of a drug on the body is the main factor in drug selection. Statins are among those medications that can cause death if taken incorrectly. To prevent severe side effects, the dosage prescribed by the doctor should not be exceeded and all his recommendations should be strictly followed.
One patient out of 100 experiences the following negative effects:
- insomnia, as well as memory impairment;
- depression;
- sexual problems.
One patient out of 1000 may experience the following side effects of the drug:
anemia;- headache and dizziness with varying intensity;
- paresthesia;
- muscle spasms;
- polyneuropathy
- anorexia;
- pancreatitis;
- disorders in the digestive tract that cause stomach pain and vomiting;
- increase or decrease in blood glucose;
- various types of hepatitis;
- allergic rashes and severe itching of the rash;
- hives;
- alopecia;
- myopathy and myositis;
- asthenia;
- angioedema;
- systemic vasculitis;
- arthritis;
- polymyalgia of rheumatic type;
- thrombocytopenia;
- eosinophilia;
- hematuria and proteinuria;
- severe shortness of breath;
- breast growth in men and impotence.
In extreme cases, rhabdomyolysis, liver and kidney failure may develop.
Features of Atorvastatin
The drug Atorvastatin belongs to the category of third generation statins. The drug is available in various dosages - 10, 20, 40 and 80 mg. The pharmacy chain offers 2 types of this drug - Russian (Atorvastatin) and Israeli (Atorvastatin-Teva). The active ingredient in Atorvastatin is atorvastatin calcium trihydrate.
The drug reduces the concentration of low-density lipoproteins and simultaneously increases the content of high-density lipoproteins. Also effective for familial and homozygous hypercholesterolemia. The effectiveness of the medicine appears after 2 weeks of regular use. After just 30 days, the maximum effect of the anticholesterol drug is achieved, which persists throughout the entire duration of treatment.
Atorvastatin, like Rosuvastatin, belongs to a new generation of statins
Taking Atorvastatin must be combined with diet. According to the diet, the patient must exclude from the diet foods rich in animal fats, as well as dishes prepared by frying. You can take the tablets regardless of meal time. The dosage is selected individually by the attending physician based on the results of the lipid profile.
The initial dosage is 10 mg; subsequently, if necessary, it can be increased to 80 mg per day. Patients suffering from renal or liver failure take Atorvastatin at this initial dosage all the time. Indications for the use of Atorvastatin are the complex treatment of high levels of total cholesterol and LDL and increased levels of triglycerides.
The following side effects may occur while taking Atorvastatin:
- sleep disturbance;
- headache and dizziness;
- anemia or thrombocytopenia;
- dyspeptic disorders;
- arthritis and myalgia;
- allergy;
- swelling;
- baldness;
- increased sweating;
- sensitivity to light.
Atorvastatin is not prescribed for use in cases of increased activity of liver enzymes, renal failure, during pregnancy and lactation, in case of individual intolerance to the components of the drug, severe liver pathologies. The drug is also contraindicated in patients under 18 years of age.
The cost of the drug in pharmacies depends on the dosage and manufacturer and varies from 130 to 400 rubles. Its analogues are the drugs Atoris, Liprimar, Tulip.
Interaction with other medications and analogues
Statins may not be compatible with all medications. Sometimes taking two medications together can cause severe side effects:
- When taken together with Cyclosporine, myopathy occurs. Myopathy also occurs when combined with antibacterial agents of the tetracycline, clarithromycin and erythromycin groups.
- A negative reaction of the body can occur when taking statins and Niacin.
If you take Digoxin and statins, the concentration of Digoxin and statins increases. It is not recommended to take statin tablets or grapefruit juice. The juice reduces the medicinal effect of the statin, but increases its negative impact on organs and systems in the body.- Parallel use of statin tablets and antacids, and magnesium, reduces the concentration of statin by 2 times. If you use these drugs at intervals of 2-3 hours, then the negative impact is reduced.
- When combining the use of tablets and protease inhibitors (HIV), then AUC0-24 increases significantly. For people infected with HIV, this technique is contraindicated and can have complex consequences.
Atorvastatin has 4 analogues, and Rosuvastatin has 12. Russian analogues “Atorvastatin-Teva”, “Atorvastatin SZ”, “Atorvastatin Canon” are distinguished by their low price and good quality. The cost of medicines is from 110 to 130 rubles.
The most effective analogues of Rosuvastatin:
- Rosucard is a Czech drug that effectively reduces cholesterol in a short therapeutic course.
Crestor is an American drug that is the original 4th generation statin drug. Crestor - passed all clinical and laboratory studies. The only drawback in it is the price of 850-1010 rubles.- Rozulip is a Hungarian medicine that is often prescribed for atherosclerosis for long-term use.
- The Hungarian drug Mertenil is prescribed to lower bad cholesterol and to prevent cardiac diseases.
Comparison of the safety of Rosucard and Atorvastatin
The safety of a drug includes many factors.
At the same time, in Rosucard it is quite similar to Atorvastatin. It is important where the drug is metabolized: drugs are excreted from the body either unchanged or in the form of products of their biochemical transformations. Metabolism occurs spontaneously, but most often involves major organs such as the liver, kidneys, lungs, skin, brain and others. When assessing the metabolism of Rosecard, as well as Atorvastatin, we look at which organ is the metabolizing organ and how critical the effect on it is.
The risk-benefit ratio is when the prescription of a drug is undesirable, but justified under certain conditions and circumstances, with the obligatory observance of caution in use. At the same time, Rosucard does not have any risks when used, just like Atorvastatin.
Also, when calculating safety, it is taken into account whether only allergic reactions occur or possible dysfunction of the main organs. In other matters, as well as the reversibility of the consequences of using Rosucard and Atorvastatin.
Comparison of side effects of Rosucard and Atorvastatin
Side effects or adverse events are any adverse medical event that occurs in a subject after administration of a drug.
Rosucard has more adverse effects than Atorvastatin. This implies that the incidence is low with Rosucard and low with Atorvastatin. Frequency of manifestation is an indicator of how many cases of an undesirable effect from treatment are possible and registered. The undesirable effect on the body, the strength of influence and the toxic effect of drugs are different: how quickly the body recovers after taking it and whether it recovers at all. When using Rosucard, the body's ability to recover faster is higher than that of Atorvastatin.
Comparison of ease of use of Rosucard and Atorvastatin
This includes dose selection taking into account various conditions and frequency of doses. At the same time, it is important not to forget about the release form of the drug; it is also important to take it into account when making an assessment.
The ease of use of Rosucard is approximately the same as Atorvastatin. However, they are not convenient enough to use.
The drug ratings were compiled by experienced pharmacists who studied international research. The report is generated automatically.
Last update date: 2021-01-10 10:02:28
Comparison of addiction between Rosucard and Atorvastatin
Like safety, addiction also involves many factors that must be considered when evaluating a drug.
So the totality of the values of such parameters as “syndrome o” for Atorvastatin is less than the similar values for Rosucard. Withdrawal syndrome is a pathological condition that occurs after the cessation of intake of addictive or dependent substances into the body. And resistance is understood as initial immunity to a drug; in this it differs from addiction, when immunity to a drug develops over a certain period of time. The presence of resistance can only be stated if an attempt has been made to increase the dose of the drug to the maximum possible.