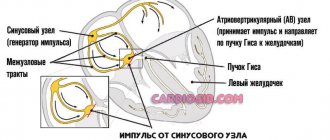
It would seem, what do the kidneys have to do with it, if in our body it is the heart that plays the role of a pump that pumps blood? But since pressure is a derivative of the work of three interdependent components, the heart, vascular tone and kidneys, in the process of evolution it so happened that the function of the pressure regulator went to the kidneys. Otherwise, they would not be able to filter the liquid entering the human body.
When this function is disrupted, the pressure drops, a large amount of a special substance, renin, begins to enter the blood, which is converted into angiotensin, which has the ability to cause vasoconstriction and stimulate the production of the adrenal hormone aldosterone. This hormone is capable of retaining sodium and water in the body, the level of circulating blood no longer corresponds to the volume of the vascular bed, which causes renal hypertension.
Causes of pathology
Increased pressure is usually associated with occlusion or stenosis of the renal artery. Against the background of pathological processes, the lumen of the vessel narrows, which leads to an increase in blood pressure. The cause of the development of this condition may be pyelonephritis, glomerulonephritis, amyloidosis, hydronephrosis, polycystic kidney disease.
The development of the disease is facilitated by systemic chronic diseases: diabetes mellitus, tuberculosis, fibromuscular dysplasia. The condition is observed with nephropathy in pregnant women.
What is this?
The symptoms and treatment of kidney pressure depend on many factors. Even young people are susceptible to this pathology. Only a doctor can find out the cause and eliminate the disease itself; it will not be possible to cope with the situation on your own.
Arterial hypertension is considered one of the most common ailments, but few people know that the kidneys are often involved in the occurrence of the disease. Malfunctions of this organ directly affect blood pressure. Doctors call this disease “renal hypertension.” The relationship between kidneys and blood pressure is very close. The job of the kidney is to regulate fluid levels in the body, as well as remove harmful and toxic substances from the body. If the kidneys do not do their job well, pressure increases in the circulatory system.
In addition, renal pressure may be below normal, which also indicates the presence of pathology in this area of the body. In this case, the water level in the body is below normal, and a mild degree of dehydration is observed.
Renal hypertension is not considered an independent disease. This condition develops under the influence of certain pathological factors that have a destructive effect on the kidneys. This situation provokes a malfunction of the organ, as a result of which there is a decrease in blood flow, sodium and water retention in the kidneys, resulting in swelling. The accumulation of sodium ions leads to swelling of the vascular walls, increasing their sensitivity.
For this reason, the organ's receptors actively produce an enzyme called renin. After certain pathological transformations, this substance affects the tone of blood vessels, reducing their patency, which will inevitably lead to an increase in pressure in this area.
Treatment for renal hypertension depends on the type of the disease. With one course, medications can help, but with another, only surgical intervention is necessary.
Classification of renal hypertension:
- Parenchymatous. Appears as a consequence of nephrogenic pathologies that cause damage to the vascular tissue of the kidney parenchyma, as well as the glomeruli of the organ.
- Vasorenal. It occurs when the arteries of the kidneys are destroyed, which causes poor blood supply to the area. It can be acquired and congenital.
- Mixed. It is diagnosed by a combination of the first two types of pathology and is considered the most dangerous form of the disease.
Half of the patients have parenchymal renal hypertension; this type of disease is the most common. The consequence of this disease can also be its progression, as a result of which the tissue of the kidney itself dies, and substances that regulate vascular tone are synthesized in smaller quantities. However, more often this development of the situation concerns elderly and senile people.
Clinical picture
Renal arterial hypertension is characterized by a significant increase in blood pressure and accompanying conditions. Patients complain of the following ailments:
- constant thirst;
- general weakness;
- lower back pain;
- frequent urination;
- increased body temperature;
- pain when urinating.
In addition, the pathology may be accompanied by discomfort characteristic of high blood pressure: headache, shortness of breath, vomiting, nausea, dizziness and blurred vision.
It is important to understand that the symptoms of renal hypertension require medical attention. Treatment based on recommendations from friends or advice from the Internet can lead to rapid progression of the disease. A serious deterioration in kidney function will be noticeable within a few months. Such conditions are very difficult to treat with medication, so timely consultation with a doctor is the key to successful therapy.
Therapy and prognosis
In the treatment of renal hypertension, absolute preference is given to surgical methods and special invasive procedures. Common treatments for renal (renovascular) hypertension:
- microprosthetics of walls (strengthening kidney tissue);
- angioplasty (during treatment, a catheter is inserted into the artery of the affected kidney, through which blood clots are removed, the lumen is increased to normalize blood flow);
- surgical treatment (surgical elimination of the causes of PG symptoms): possible with partial preservation of the functionality of the organ;
- therapeutic treatment of the underlying disease with elimination of the symptoms of hypertension through pharmacology.
During treatment, it is not recommended to direct the main efforts to equalize blood pressure, against the background of which renal hypertension occurs. This is the only case when treatment of hypertension can be delayed (until the pressure in the kidneys is restored).
Diagnostics
In most cases, patients complain of high blood pressure. If the condition is accompanied by lesions of the renal parenchyma or its vessels, the doctor raises the question of the renovascular nature of the disorder. For diagnosis, the specialist prescribes the following studies:
- clinical blood test;
- general urine analysis;
- blood biochemistry;
- Reberg's test;
- excretory urography;
- Ultrasound of the kidneys;
- Dopplerography of renal vessels;
- arteriography and aortography of the renal vessels;
- spiral CT or MRI.
If kidney cancer is suspected, the specialist will insist on a biopsy and histological examination.
Provocateurs PG
Professional instrumental and laboratory diagnostics should be urgent (at the first symptoms of dysfunction) for three reasons.
- In 80% of cases, renal hypertension develops quickly and is accompanied by damage to all target organs.
- Without urgent diagnosis of the causes of the disease, therapeutic treatment of symptoms is unsuccessful in 20% of cases.
- The prognosis for renal hypertension is 55% negative, but early diagnosis increases the chance of recovery.
The causes of hypertension are divided depending on its types. There are three forms of hypertension:
- Parenchymatous (caused by damage to the parenchyma). In the diagnosis of renal hypertension, common pathogens are nephropathy, neoplasms (cysts, tumors), tuberculosis, inflammation (glomerulonephritis, pyelonephritis). Requires urgent treatment of the provoking disease.
- Vasorenal renal hypertension is the result of deformation of the renal vessels against the background of symptoms of thrombosis, atherosclerosis, and disruptions in the blood supply system. Symptoms develop quickly, treatment is predominantly surgical.
- A mixed form of hypertension, accompanied by symptoms of kidney pathologies and blood flow disorders.
Renal parameters of biochemical blood tests
For some, biochemical blood test indicators allow the doctor to draw a conclusion about the condition of the kidneys. The analysis is carried out in the morning on an empty stomach. Preparation for the study is as follows:
- the day before the collection of biological material, alcohol intake is excluded;
- at least 12 hours must pass between blood collection and the last meal;
- one hour before the test, you need to stop smoking;
- Before the test, you can only drink water.
Let's look at the main research indicators that help detect kidney disease.
Creatinine
The substance, which is formed in muscle tissue, then enters the blood and is excreted from the body by the kidneys. The primary task of creatinine is to provide the body with the energy necessary for muscle contraction. The level of the substance in the blood largely depends on muscle mass. That is why its concentration in the blood of men is higher than that of women and children.
Creatinine is a non-threshold substance that does not undergo reabsorption in the renal tubules and is completely excreted by the urinary system at any concentration in the blood. With stable muscle load and good kidney function, its concentration in a person’s blood is quite constant. Therefore, the level of creatinine in the blood directly reflects the functional state of the kidneys.
Reference values of the indicator are presented in the table ⇓⇓⇓
| Age | Creatinine level, µmol/l |
| <1 year | 18-35 |
| 1-14 years | 35-110 |
| Men | 80-115 |
| Women | 53-97 |
High levels of the substance in the blood may indicate the following kidney diseases:
- acute renal failure - a rapidly developing disorder of the kidneys;
- chronic renal failure - gradual decline of renal function;
- glomerulonephritis - damage to the glomeruli, which may be a consequence of infection or an autoimmune process;
- pyelonephritis is an inflammatory process in the renal tubules.
Also, the cause of a high rate may be ureteral obstruction caused by an inflammatory process or a mechanical factor. For example, obstruction can occur with urolithiasis. If a stone enters the ureter, the outflow of urine is disrupted, and accordingly the level of creatinine in the blood increases.
A high level of the indicator does not always indicate kidney problems. The concentration of the substance in the blood increases with fever, injuries with tissue destruction, dehydration, severe physical exertion, and the predominance of meat products in the diet. Also, increased creatinine values can be observed with hyperthyroidism, acromegaly, and gigantism.
Low values are observed in the early stages of pregnancy, with prolonged fasting or lack of meat products in the diet, or excess water content in the body.
Urea
The formation of urea occurs in several stages:
- The breakdown of proteins produces ammonia, a substance toxic to the body.
- Ammonia is neutralized by liver cells, turning into urea, which is excreted from the body by the kidneys.
The body does not use this chemical compound in any way, but only gets rid of it. Since the process of urea formation is continuous, a small amount of the substance is constantly in the blood. Reference values of the indicator are presented below ⇓⇓⇓
As a rule, an increase in urea levels in the blood is caused by the same factors as an increase in creatinine levels. But low levels most often indicate liver pathologies. The indicator also decreases with nephrotic syndrome, low-protein diet, overhydration, and in early pregnancy.
Uric acid
It is formed as a result of the exchange of purines - nitrogen-containing substances that make up nucleic acids. In addition, uric acid is a result of the digestion of foods high in purines. Most of the substance is excreted from the body by the kidneys, a smaller part by the gastrointestinal tract. Reference values for uric acid levels in the blood are presented in table ⇓⇓⇓
An increase in the indicator may be a sign of kidney failure, as well as:
- gout - deposits of urate crystals in the tissues;
- Lesch-Nychen syndrome - a hereditary pathology in which the synthesis of uric acid is increased;
- malignant diseases of the hematopoietic system;
- alcohol intoxication of the body;
- taking diuretics;
- the predominance in the diet of foods rich in purines - fish, veal, offal, legumes;
- excessive physical activity.
A low rate is observed with renal tubular dysfunction. For example, the level of uric acid in the blood decreases in Fanconi syndrome, a hereditary disease characterized by a general disorder of proximal tubular transport.
Other reasons for low levels are disorders of purine metabolism and a low-purine diet.
Total protein
The indicator reflects the concentration of all proteins in the blood and serves as a marker not only of kidney pathologies, but also diseases of the liver, thyroid gland and other organs. The reference values of the indicator are as follows ⇓⇓⇓
High levels of total protein in the blood are observed with:
- dehydration of the body;
- acute and chronic infectious pathologies;
- autoimmune processes;
- malignant formations.
Low values of the indicator may indicate glomerulonephritis, nephrotic syndrome. In addition, the concentration of protein in the blood decreases with liver diseases, bleeding, hyperfunction of the thyroid gland, fasting, during pregnancy, and during breastfeeding.
Glomerular filtration rate (GFR), Rehberg test
Nephrons (the structural units of the kidney) consist of glomeruli and tubules. The first stage of urine formation occurs in the renal glomeruli - filtration of almost all components of plasma, except for high-molecular proteins and blood cells. Reverse reabsorption of some substances occurs in the renal tubules, i.e. tubular reabsorption reflects the state of the renal concentration function.
In some kidney pathologies, this process is disrupted.
To assess the functional state of various parts of the nephron, several methods are used: determining GFR and performing the Rehberg test. GFR is calculated using a special formula that reflects the patient's age, gender, weight, height, race, and the individual's blood creatinine level.
Rehberg test - the test reflects several indicators: GFR, tubular reabsorption and minute diuresis. There are several options for conducting a test:
- The daily amount of urine is collected. The first morning portion of urine is passed into the toilet, and the time of urination is recorded. All daily urine, including the morning portion of the next day, is collected in a sterilized container with a capacity of 2-3 liters. The last urination should coincide with the time noted the day before. During the collection of biological material, the container with urine should be stored in the refrigerator, but not frozen. After collecting the last portion of urine, the total volume of urine is measured. The biological material is mixed, and approximately 30-50 ml is taken from it into a small container; the container is marked, indicating the daily volume of urine. For example: “Diuresis 1100 ml.” The biological material is delivered to the laboratory as quickly as possible, where blood is also drawn from a vein.
- Currently, the most commonly used option is one that does not require collecting a daily amount of urine. A two-hour portion of urine is collected and blood is taken from the patient’s vein during this period of time. In the laboratory, the level of creatinine in urine and blood is determined and the indicators of minute diuresis, GFR, and tubular reabsorption are calculated using special formulas.
Reference values for creatinine clearance are presented in the table, units of measurement are ml/min/1.7 m².
The accuracy of the research results largely depends on proper preparation. In this regard, a few days before the start of urine collection, you need to exclude:
- strong physical activity;
- consumption of alcoholic beverages, caffeine;
- taking diuretics, drugs containing ascorbic acid.
It is also worth limiting your consumption of meat products.
What diseases can the study detect?
- The study of glomerular filtration is of great practical importance, since in a number of renal pathologies (chronic glomerulonephritis, lupus nephritis, diabetic glomerulosclerosis), a decrease in GFR is the earliest sign of incipient chronic renal failure.
- High GFR values are a sign of nephrotic syndrome, the onset of diabetes mellitus, and arterial hypertension.
- Also, the indicator may deviate from the reference values for physiological reasons. For example, an increase in GFR is observed with excess protein in the diet, taking diuretics, and drinking plenty of fluids; decrease - with dehydration, with a salt-free diet.
- A decrease in tubular reabsorption occurs early in patients with polycystic kidney disease, hydronephrosis, and pyelonephritis. In kidney diseases accompanied by predominant damage to the glomeruli (glomerulonephritis, etc.), tubular reabsorption decreases much later than glomerular filtration.