Takayasu's disease (Takayasu syndrome, aortic arch syndrome, nonspecific aortoarteritis) is a granulomatous inflammation of the aorta and its large branches and their stenosis. The disease was first described by Japanese ophthalmologist Mikito Takayasu in 1908. The disease mainly affects women. The average age of cases in Europe reaches 41 years, in Japan - 29, in India - 24. It is most common in Japan, Southeast Asia, India and Mexico. There are no exact data on the prevalence in Russia. In children, the disease has a more acute and aggressive course.
Story
In the first descriptions, nonspecific aortoarteritis was called “pulseless disease” - because due to obliteration of the large branches of the aorta, patients often had no pulse in the upper extremities.
Before the official discovery, the most similar disease was described by the professor of anatomy at the University of Padua Giovanni Batista Morgagni (1682–1771) in 1761: in a woman aged about forty years, an autopsy revealed dilation of the proximal part of the aorta in combination with stenosis of the distal parts, the inner layer of the aorta was yellow in color and contained calcifications. During life, the patient had no pulse in the radial arteries.
In 1839, British military doctor James Davy described another similar case. A 55-year-old soldier at the age of 49 developed pain in his left shoulder, and four years later the pulse in his hand weakened, for which he consulted a doctor. A year later, the man suddenly died; an autopsy revealed a large rupture of the aortic arch aneurysm and complete occlusion of the vessels extending from the aortic arch.
In 1854 in London, surgeon William Savory (1826–1895) also reported a disease very similar to Takayasu's disease. In a 22-year-old woman, no pulse was detected in the vessels of the neck, head and upper extremities for five years; seizures began to occur during the course of the disease, and the patient died. An autopsy revealed thickening and narrowing of the aorta and arch vessels - they felt like a thick rope to the touch, there were no aneurysms.
Finally, in 1908, the Japanese ophthalmologist Makito Takayasu, at the Twelfth Annual Conference of the Japanese Society of Ophthalmology, reported on two annular anastomoses around the optic disc in a young woman without pulses in the peripheral arteries. These were arteriolovenular shunts. In addition, the blood vessels surrounding the optic disc were slightly elevated. Japanese colleagues associated changes in retinal vessels with the absence of pulses in the patient’s radial arteries.
Pulselessness syndrome has been called by many names, leading to confusion. It was only in 1954 that Japanese doctors William Caccamise and Kunio Okuda introduced the term “Takayasu disease” (TD) into the English literature.
Complications and prognosis
With Takayasu's disease, complications occur at a fairly young age. The most expected and difficult ones are:
- myocardial infarction;
- spinal cord infarction;
- ischemic stroke;
- aortic aneurysm dissection;
- blindness.
The course of the disease is long-term. With full treatment, a five-year survival rate of 80% of patients is achieved. It has been established that symptomatic renal hypertension develops in 33–83% of patients. It worsens the clinical course and prognosis, and reduces 10-year survival rate by 15%.
Kidney amyloidosis complicates the pathology quite rarely; it is characterized by nephrotic syndrome with impaired excretion and reabsorption of protein and other useful substances and a high concentration of residual nitrogen. Treatment requires the use of hemodialysis. The average life expectancy for this complication is up to five years.
Since the causes are unclear, there are no primary preventive measures. Secondary recommendations include the doctor’s requirement to sanitize all chronic foci of infection, limit contact during an outbreak of influenza and ARVI, and take immunocorrectors.
Takayasu's disease is a rare pathology, but attending physicians need to remember it. This is especially true for young patients who present with many diverse complaints. Timely examination will help make a diagnosis. Neglect of one's health among young people develops into incorrigible forms of pathology at a more conscious age.
Etiology and pathogenesis of Takayasu syndrome
Most often, the cause of BT cannot be determined; a connection with tuberculosis and streptococcal infections is assumed. There is evidence of an increased frequency of a number of histocompatibility antigens in patients in various populations:
- India - HLA B5, B21;
- USA - HLADR4, MB3;
- Japan - HLADR2, MB1, Bw52, DW2, DQW1 HLA Bw52‑CAD, AR, HLA B39.
Autoimmune mechanisms play a certain role in the pathogenesis: there is an increase in the level of IgG and IgA and fixation of immunoglobulins in the wall of the affected vessels. Also characteristic are changes in the cellular component of immunity and disturbances in the rheological properties of blood with the development of chronic disseminated intravascular coagulation syndrome.
The course of Takayasu disease (TD) has a certain stage. At an early stage of the disease or during exacerbations, nonspecific symptoms of systemic inflammation occur. During this period, up to 10% of patients do not have any complaints at all. As it progresses, there is inflammation of the vessel walls and the development of stenosis, which almost always occurs, even in patients with aneurysms. Bilateral vascular stenosis predominates.
Diagnostics
A rheumatologist, neurologist, and vascular surgeon are involved in making a diagnosis, taking into account the diverse clinical picture.
Criteria have been developed to more likely assess symptoms. Their specificity is about 98%. To diagnose nonspecific aortoarteritis, three or more possible manifestations must be present:
- the onset of the disease should occur at a young age;
- in the hands there are signs of the syndrome in the form of “intermittent claudication”;
- peripheral pulsation is weakened or absent;
- By measuring blood pressure in both arms, a difference of more than 10 mmHg is determined. Art.;
- upon auscultation of the area of the abdominal aorta and subclavian artery, characteristic noises are heard;
- The angiogram confirms anatomical changes in the vessels.
Arm pain may be accompanied by cramps
In the blood test:
- moderate anemia;
- leukocytosis;
- acceleration of ESR;
- decreased level of γ-globulins;
- at the same time it is possible to reduce the concentration of cholesterol, lipoproteins, albumins, seromucoid, haptoglobin.
Immunological studies do not necessarily show growth of antibody complexes.
No changes are found on the x-ray of the joints.
The rheoencephalography method determines a decrease in blood supply to the brain, and using an electroencephalogram, a decrease in the functional activity of cortical cells can be determined.
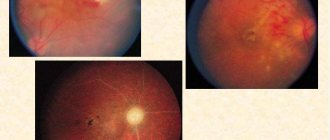
In the fundus of the eye, the ophthalmologist detects retinopathy and damage to the optic nerve
Angiography and aortography can reveal stenosis of the arteries; combinations with atherosclerosis are often found.
Ultrasound diagnostics and Doppler sonography establish disturbances in blood flow, changes in arterial walls, the degree of stenosis, its localization and segmental nature.
A biopsy in the early stages reveals a typical nature of inflammation with granulomatous growths, attraction of immune cells (lymphocytes, giant multinucleated macrophages). In the late stage, identifying a sclerotic vessel has no diagnostic value.
Clinical picture: symptoms of Takayasu's disease
In the acute stage, patients are most often bothered by nonspecific symptoms of systemic inflammation. These are fever, night sweats, malaise, weight loss, joint and muscle pain, and moderate anemia. But already at this stage there may be signs of vascular insufficiency, especially in the upper extremities - absence of pulse. The absence of a pulse or a decrease in its filling and tension in one of the arms, asymmetry of systolic blood pressure in the brachial arteries is recorded in 15–20% of cases. Much more often, in 40% of cases, patients complain of a feeling of weakness, fatigue and pain in the muscles of the forearm and shoulder, often unilateral, aggravated by physical activity. At this stage, BT is diagnosed extremely rarely.
The chronic stage, or the full picture stage, begins after 6–8 years. Symptoms of damage to the arteries extending from the aortic arch predominate due to the progression of inflammation of the vessel walls and the development of stenosis, usually bilateral. Even in the presence of an aneurysm, in almost all cases there is also stenosis. As stenosis progresses, symptoms of ischemia of individual organs appear. Vascular inflammation can occur without systemic inflammatory reactions, then pain is observed at the site of projection of the affected vessel or tenderness upon palpation.
On the affected side, increased fatigue of the arm develops during exercise, its coldness, a feeling of numbness and paresthesia, the gradual development of atrophy of the muscles of the shoulder girdle and neck, weakening or disappearance of the arterial pulse, a decrease in blood pressure, in 70% - a systolic murmur is heard in the common carotid arteries. 7–15% of patients experience neck pain, dizziness, transient moments of visual impairment, shortness of breath and palpitations, and 15% of patients experience pain on palpation of the common carotid arteries (carotidynia).
During this period, compared with the early stage of the disease, symptoms of vascular insufficiency of the upper extremities and intermittent claudication, damage to the cardiovascular system, brain and lungs are much more common (50–70%).
Publications in the media
Takayasu's disease is a chronic inflammatory disease of the aorta and its branches, less commonly the pulmonary artery, with the development of stenosis or occlusion of the affected vessels and secondary ischemia of organs and tissues. Statistical data. Frequency - from 1.2 to 6.3 per 1,000,000 population per year. Until 1955, only 100 cases of the disease were described in the world literature. The predominant gender is female (15:1). Most often occurs at a young age (from 10 to 30 years). The disease is more often observed in Asia and South America, less often in Europe.
Etiology unknown.
Pathogenesis and pathomorphology. Damage to the endothelium and local thrombus formation leads to the deposition of immune complexes. The likelihood of thrombotic complications increases in the presence of antibodies to phospholipids.
Against the background of inflammation in the walls of blood vessels, atherosclerotic changes in various phases are often detected. The proximal segments of small and medium caliber arteries are affected. Damage to the arteries of internal organs is not typical.
Classification • Damage to the aortic arch and its branches (8%) • Damage to the thoracic and abdominal aorta (11%) • Damage to the arch, thoracic and abdominal aorta (65%) • Damage to the pulmonary artery and any part of the aorta.
Clinical picture • General symptoms: weight loss, weakness, fever (40%) indicate an active phase of the disease • Aortic arch syndrome •• Absence of pulse in the left radial artery •• Episodes of cerebral ischemia or stroke •• Ophthalmological manifestations: narrowing of visual fields, decreased acuity vision, diplopia, retinal vascular aneurysms, hemorrhages, retinal detachment (rare), cataracts, loss of vision (sometimes temporary) • Vascular insufficiency syndrome of the upper extremities caused by blockage of the subclavian arteries: pain in the extremities, chilliness, muscle weakness, trophic disorders. Physical findings: ••• absence of pulsation (or its weakening) below the site of arterial occlusion (or stenosis) ••• presence of systolic murmur above the site of stenosis and somewhat distally ••• difference in blood pressure in both arms ••• Raynaud's syndrome • Syndrome insufficient blood supply to the face and neck; trophic disorders have been described, including gangrene of the tip of the nose and ears, perforation of the nasal septum, atrophy of the facial muscles • Syndrome of insufficient blood supply (“intermittent claudication”) of the lower extremities: pain, fatigue in the proximal extremities during physical activity. Physical data: weakened pulsation, systolic murmur over the affected vessels • Arterial hypertension syndrome of the renovascular type due to involvement of the renal arteries in the process • Skin lesions: erythema nodosum, leg ulcers • Joint damage ••• Arthralgia ••• Migratory polyarthritis with predominant damage to the upper joints limbs • Heart damage ••• Damage to the proximal sections of the coronary arteries with the development of ischemic syndrome up to MI ••• Myocarditis ••• Aortic valve insufficiency ••• Heart failure • Lung damage ••• Pulmonary hypertension (type IV Takayasu disease) • Lesion kidneys: glomerulonephritis, amyloidosis (rare).
Laboratory data • An increase in ESR marks the active (inflammatory) stage of the disease • OAM without pathology • RF, ANAT, AT to cardiolipin are rarely detected.
Instrumental data • X-ray examination of the joints - articular pathology is not detected • Aortography, selective angiography of the affected vessels reveals incomplete and complete occlusions of the branches of the aortic arch, varying in location and extent • Magnetic resonance angiography • Dopplerography of vessels • Biopsy in the early stages reveals a granulomatous inflammatory reaction with involvement of lymphocytes, macrophages, giant multinucleated cells. The sclerotic phase is not specific, and in this case the biopsy is not informative.
Diagnostic criteria (American College of Rheumatology) • Age less than 40 years • Intermittent claudication of the lower extremities • Weak radial pulse • Difference in systolic blood pressure between the right and left brachial arteries of more than 10 mm Hg • Murmur over the subclavian arteries or abdominal aorta • Angiographic changes: narrowing or occlusion of the aorta and/or its branches, not associated with atherosclerosis, fibromuscular dysplasia or other causes • The diagnosis is considered reliable if 3 or more criteria are present. Sensitivity - 90.5%, specificity - 97.8%.
Complications • MI • Stroke • Aortic aneurysm dissection.
Features in pregnant women. Pregnancy should be planned during the period of remission of the disease, provided that cytotoxic immunosuppressants are not used. During pregnancy, hypertensive syndrome may increase, which has adverse consequences for both the fetus and the mother.
TREATMENT
General tactics include immunosuppressive therapy in the active stage of the disease, as well as correction of hemodynamic changes.
regimen is selected individually, taking into account the adaptive capabilities of the vascular bed of the heart and limbs. Diet. In case of arterial hypertension, it is necessary to limit the amount of salt in the diet.
Drug treatment
• Prednisolone is the basis of treatment in the active phase. Prescribe 40–60 mg/day, then the dose is gradually reduced to maintenance (5–10 mg/day).
• Immunosuppressants are added if there is no effect from GC monotherapy. Methotrexate 7.5–25 mg/week is usually used.
• Antihypertensive drugs (except for ACE inhibitors, contraindicated in renal artery stenosis) • Antiplatelet agents (dipyridamole, acetylsalicylic acid) and indirect anticoagulants have been proposed for the secondary prevention of thrombotic complications, but there is no evidence of the advisability of their use.
Surgery
• Indications for angioplasty: •• renal artery stenosis with symptomatic hypotension •• coronary artery stenosis with ischemic syndrome •• intermittent claudication syndrome •• critical stenosis of 3 or more cerebral vessels •• aortic valve insufficiency •• aneurysmal dilatation of the thoracic or abdominal aorta more than 5 cm in diameter.
• Methods of surgical treatment: •• endarterectomy (usually with expansion of the lumen of the vessel with a patch) for isolated segmental occlusions of the main arteries arising directly from the aorta •• bypass with synthetic vascular prostheses for occlusions over a significant extent and multiple lesions •• percutaneous angioplasty is indicated for single stenotic vascular changes.
Prognosis • The course is usually long-term • Rapidly progressive forms are usually observed at a young age • The development of myocardial infarction, stroke, retinopathy significantly worsens the prognosis.
Synonyms • Pulseless disease • Inverted coarctation of the aorta • Panarteritis multiplex obliterans • Aortic arch syndrome • Takayasu syndrome.
ICD-10 • M31.4 Aortic arch syndrome [Takayasu].
Damage to internal organs
In the chronic stage, symptoms sometimes appear due to damage to the arteries arising from the abdominal aorta, most often with anatomical types II and III of the disease. Vasorenal arterial hypertension of a malignant course, attacks of “abdominal toad” caused by damage to the mesenteric arteries, intestinal dyspepsia and malabsorption may develop.
Clinical signs of lung damage (chest pain, shortness of breath, nonproductive cough, rarely hemoptysis) are observed in less than a quarter of patients.
Damage to the coronary arteries occurs in ¾ of patients, in 90% of cases the mouths of the coronary vessels are affected, and the distal parts are rarely affected. Damage to the ascending aorta is often described - compaction combined with dilatation and the formation of aneurysms. Arterial hypertension occurs in 35–50% of cases and can be caused by involvement of the renal arteries or the development of glomerulonephritis, less often by the formation of coarctation of the aorta or ischemia of the vasomotor center against the background of carotid vasculitis. As a result of arterial hypertension, coronaryitis and aortic regurgitation, chronic heart failure develops.
Anatomical variants of Takayasu's disease:
Type I - the lesion is limited to the aortic arch and its branches (8% of patients); Type II - the descending part (thoracic and abdominal sections) of the aorta is affected (11%); Type III (mixed) - the most common, includes damage to the aortic arch and its descending section (65%); Type IV - includes lesions characteristic of the first three options in combination with arteritis of the branches of the pulmonary artery; occlusion of the brachial and iliac arteries, damage to the aortic arch and renal arteries is also observed (Takayasu-Denerey syndrome, 16%).
Pathomorphology
In the chronic phase, the aorta is thickened due to fibrosis of all three layers of the vessel. The lumen often narrows in several places. If the disease progresses quickly, fibrosis does not have time to lead to the formation of an aneurysm. The intima may be ribbed, with a “tree-bark” appearance; this feature is characteristic of many aortoarteritis. These changes usually occur in the aortic arch and its branches, but the thoracic and abdominal parts of the aorta and their corresponding branches may be involved in the process.
Recent studies of the cellular composition of the aortic walls have shown that the formation of new vessels occurs in the deep intima associated with the adventitia. T cells and dendritic cells are also observed in the vascular environment, with small numbers of B cells, granulocytes and macrophages. Inflammation is most noticeable in the adventitia, with infiltration of B and T cells.
As a result, ischemia, hypertension, and atherosclerosis develop. With a slow course, there is a pronounced development of collateral circulation.
Pathological changes in blood vessels and pathogenesis
In Takayasu's disease, a disorder is found in the wall of the aortic arch and large vessels extending from it. Morphological changes go through several stages:
- In the initial period, the inflammatory process consists of the formation of granulomas (clusters of cells) from monocytes, lymphocytes, macrophages and a small number of giant multinucleated cells. They are located in the inner and middle membranes of arteries with a caliber of 1.5 cm or more and in their own vessels feeding the wall.
- Next, the granulomas transform into fibrous and destroy muscle fibers.
- In response to necrosis, mucopolysaccharides and collagen accumulate, thickening of the inner and middle layers occurs, and smooth muscle cells proliferate.
- In the final stage, all layers of the wall are replaced by fibrous tissue, and increased parietal thrombus formation is possible as contractility decreases.
Histologists call the inflammatory process panarteritis. Due to it, the lumen narrows, blood flow in the internal organs decreases.
The arrows indicate areas of narrowing and aneurysms that are most characteristic of Takayasu's disease.
Typical changes are multiple segmental stenoses. They alternate with unchanged vascular tissues. Sclerotic areas expand, form small aneurysms and irregularities. Most often the pathology is localized in the initial sections:
- aortic arch,
- internal carotid arteries,
- vertebral and subclavian arteries.
It is rare to find typical changes in:
- pulmonary vessels,
- renal,
- iliac arteries (a variant of Takayasu-Dereney syndrome).
It is believed that the basis of the pathogenesis of nonspecific aortoarteritis lies in autoimmune processes. But how important their role is is still unclear.
Areas of inflammation leading to disruption of brain supply
Treatment of nonspecific aortoarteritis
Taking steroid medications is the main treatment for Takayasu's disease. Data on its effectiveness vary, which may be related to the stage of the disease. Data obtained in the USA in 1985 showed that in six out of 29 patients, steroid treatment led to a decrease in ESR, inflammatory symptoms. Eight of the 16 patients with absent pulses experienced their return after a delay of several months. Later (1994) American studies showed that remission was achieved in 60% of cases (out of 48 patients).
It is now generally accepted that approximately half of patients treated with steroids experience improvement. The lack of universal treatment and the side effects associated with steroid use have led to the search for more effective treatments.
As with other systemic vasculitides, immunosuppressive drugs can be used, including cyclophosphamide, azathioprine, and methotrexate. American researchers in 1994, using the example of 25 patients who were not amenable to treatment with steroid drugs, showed that taking cytostatic drugs (cyclophosphamide, azathioprine or methotrexate) leads to remission in 33% (Takayasu arteritis. Ann Intern Med 1994;120:919– 29).
Since methotrexate is easily tolerated, its effectiveness in combination with steroids was further studied. Thirteen of 16 study participants with aortic arch syndrome taking methotrexate (81%) experienced remission. However, 7 of them experienced relapses when they completely stopped taking steroid drugs. Ultimately, eight patients experienced sustained remission for four to 34 months, and four of them were able to stop treatment completely. In three of the 16, the disease progressed despite treatment.
Thus, about a quarter of patients with active disease do not respond to current treatments.
Complications
Aortic arch syndrome can vary in severity. In some people, the disease is mild and is not accompanied by complications. However, in other cases, prolonged or repeated cycles of arterial inflammation and healing can lead to one or more of the following:
Reduced elasticity and narrowing of blood vessels, which can lead to a decrease in blood supply to organs and tissues. Arterial hypertension, which usually develops as a result of decreased blood supply to the kidneys. An inflammatory process in the heart that can affect the heart muscle (myocardium), the heart valves (valvulitis) or the sac around the heart (pericarditis). Heart failure due to hypertension, myocarditis, or aortic regurgitation—a condition characterized by blood leaking back into the heart due to a leaky aortic valve—or a combination of these conditions. Ischemic stroke is a type of stroke that occurs when blood flow in the arteries leading to the brain is reduced or blocked. Transient ischemic attack, a temporary disorder of cerebral circulation, the symptoms of which are identical to those of an ischemic stroke, but does not cause long-term damage. An aortic aneurysm, which occurs when the walls of a blood vessel weaken and bulge, forming a bulge in the vessel that can rupture. A heart attack (myocardial infarction) is an uncharacteristic phenomenon that can develop as a result of a decrease in blood supply to the heart. Damage to the lungs when the disease develops in the arteries leading to the lungs (pulmonary arteries) Pregnancy
In women with aortic arch syndrome, uncomplicated pregnancy is possible. However, the disease can negatively affect a woman's reproductive ability and the course of pregnancy. If you have aortic arch syndrome and are planning a pregnancy, it is important to work out a detailed action plan with your doctor before becoming pregnant to prevent possible complications. In addition, during pregnancy it is necessary to be under close medical supervision.
Surgery
It is advisable to perform surgical intervention on the aorta and great vessels in the first five years after diagnosis.
- Endarterectomy is indicated for small occlusions.
- Bypass surgery with special prostheses is performed when the lesion is large.
Indications for surgery are determined by the extent of the process and the degree of obstruction of peripheral vessels. Surgery is performed outside the active stage of BT.
Clinical example
A 13-year-old girl was admitted to the pediatric department on the referral of a cardiologist with complaints of headaches, nosebleeds, and increased blood pressure to 220/110 mm.
rt. Art. She did not suffer from childhood infections. Vaccinated according to age up to three years. From the age of nine she was in a boarding school (her mother and father abused alcohol and were deprived of parental rights). At the age of ten, myopia was detected (wears glasses). For the last two years, the child has been under the care of her aunt, who considers the girl sick since she was nine years old, when the above-described complaints appeared. Upon admission to the department, the girl’s condition was of moderate severity, the child had an asthenic build and poor nutrition. During auscultation of the heart, a systolic murmur is heard at the V point. The liver is 1 cm below the edge of the costal arch, blood pressure is at the level of 180–150/85–80.
The hemogram shows slight neutrophilia, ESR - 43 mm/h. In a biochemical blood test, C-reactive protein was elevated, the rest was without pathology, antistreptolysin-O and rheumatoid factor were not detected. Coagulogram - decreased prothrombin index. ECG without pathology. EchoCG revealed moderate hypertrophy of the interventricular septum and posterior wall of the left ventricle, left-sided aortic arch, narrowing of the aorta in a typical location to 5–6 mm. According to CT/MRI, there are signs of Takayasu's disease (type IV): intimal detachment of the ascending aorta with transition to the arch, segmental stenosis of the thoracic descending aorta, damage to long segments of the great vessels of the brain, CT data in favor of segmental narrowing of the left renal artery.
Metipred and methotrexan were prescribed. Symptomatic therapy included aspirin, atenolol, chimes, and captopril. During therapy, regression of general inflammatory signs was noted, but hypertension could not be completely suppressed. Three months later, the dose of metipred was increased, antihypertensive therapy was adjusted, but the pressure remained high. Taking into account the nature of vascular damage (type IV), the unstable and partial anti-inflammatory effect of the therapy, in this case the prognosis for life is very unfavorable.
Adapted from: Okhotnikova E.N. et al.: Takayasu’s disease (nonspecific aortoarteritis) is a fatal systemic vasculitis in children. "Clinical immunology. Allergology. Infectology", No. 2, 2011.
1.General information
Takayasu aortoarteritis (Takayasu disease, Takayasu syndrome, nonspecific aortoarteritis, sometimes in web sources you can also find the erroneous spelling “Takayasu arthritis”) is a granulomatous inflammatory process that affects large blood vessels, namely the arteries of the main aorta. Interestingly, this disease was first mentioned and described by ophthalmologists (it was named after its discoverer) more than a hundred years ago - as an unusual inflammation of the retinal vessels.
Today, Takayasu's disease is considered one of the rarest diseases, but by all criteria it is precisely a disease, a pathological process with certain patterns, and not sporadic unsystematic accidents. The frequency of occurrence is, according to various estimates, 1-4 people per million; Despite great difficulties in collecting the necessary statistics, it has been reliably established that women get sick approximately eight times more often than men, and the most common age of manifestation varies between 15-40 years.
A must read! Help with treatment and hospitalization!
Exodus
The 5- to 10-year survival rate for Takayasu disease is about 80%, and the five-month to one-year survival rate is close to 100%. The most common cause of death is stroke (50%) and myocardial infarction (about 25%), less often - rupture of an aortic aneurysm (5%). With damage to the coronary arteries in the first two years from the onset of symptoms of cardiac pathology, mortality reaches 56%. An unfavorable prognosis in patients whose disease is complicated by retinopathy, arterial hypertension, aortic insufficiency and aortic aneurysm. Patients with two or more of these syndromes have a 10-year survival rate from diagnosis of 59%, with most deaths occurring in the first five years of the disease.
Contraindications to surgery for aortoarteritis are the acute period of myocardial infarction, stroke, chronic renal failure, sepsis, diabetes mellitus and obliteration of distal vessels.
2. Reasons
For a long time, the causes of aortic-arterial inflammation remained completely unclear. Today, most experts are inclined to believe that Takayasu’s arteritis is one of the autoimmune rheumatoid diseases in which the body’s defense system begins to attack and tries to destroy its own cells, recognizing them as foreign. However, this hypothesis, for all its validity (the obvious clinical and pathomorphological similarity with diseases of this type is also confirmed by laboratory results), also explains little, since science still does not have a clear and comprehensive answer to the main question: why, in fact, does it start? autoimmune attack and why in different cases it targets different organs - in particular, the walls of the blood supplying arteries, as in this case.
Visit our Rheumatology page