1.General information
The connection between the condition of the kidneys, blood pressure and characteristic swelling has been known for a long time, and not only to doctors. Seeing a pale man with bags under his eyes, rubbing his temples or the back of his head with his fingers, the most discerning among us will immediately ask: is it from the kidneys?
Indeed, in many cases, high blood pressure is caused by kidney dysfunction, and vice versa: lack of blood supply, for example, with atherosclerosis of the renal arteries, leads to damage to the nephron parenchyma (the main tissue of the kidneys, consisting of millions of filtering elements called nephrons) and chronic renal failure.
These processes are complex even for a specialist; research in this area continues, but the widespread prevalence of this type of pathology creates the need to understand at least the basic terms and modern ideas about “renal pressure.”
Arterial hypertension (AH, persistent excess of blood pressure above the conditional threshold of 140/90, hypertension) is classified into two main groups. Essential or primary hypertension is an independent polyetiological disease, against the background of which numerous disorders and complications develop. On the contrary, secondary (symptomatic) hypertension is itself a complication of any pathological process or condition.
Statistical estimates regarding various types of hypertension vary widely, but it is known that the absolute majority of hypertension (up to 95%) are primary.
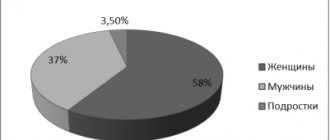
Regarding secondary hypertension, there are also no clear statistical data or generally accepted classification. The role of renal pathology in this regard is one of the main causes of symptomatic hypertension; According to various estimates, nephrogenic hypertension accounts for from 1-2% to a third of all secondary hypertension. A number of studies highlight an alarming age-related trend: persistent hypertensive blood pressure levels are found in 20-30% of children and adolescents, which is also associated with kidney dysfunction, and in cities this trend is twice as pronounced as in rural areas.
And finally, a few words about terminology. Secondary nephrogenic (renal) hypertension is an indication only of the general cause of high blood pressure; this diagnosis, in fact, is not complete and not specific. The term “renal hypertension” comes from the name of the substance “renin” discovered at the end of the 19th century (in Latin, “kidney” - ren). Renin is a vasopressor produced by the renal glomeruli, i.e. hormone that increases blood pressure. However, the definition of “renal” cannot be considered complete, because An excess of renin in the blood can be caused by both its hypersecretion and disturbances in biochemical processing due to damage to the parenchyma. Therefore, in the literature today one can find clarifying diagnoses of “renoparenchymal”, “renovascular”, “vasorenal” hypertension.
A must read! Help with treatment and hospitalization!
Hypertonic disease
Etiology:
In its development, a complex of risk factors is of direct importance. Let's look at some of them.
- Hereditary predisposition . Those whose relatives suffered from hypertension have a greater predisposition to developing hypertension.
Genetic predisposition includes:
- A membrane defect is a structural feature of cell membranes in which the permeability of the membrane to Na increases along with the rate of release of K and Ca from the cells. As a result, the cells lose K and Ca, the sensitivity of SMCs to catecholamines increases, which, together with an increase in intracellular Na (makes the cell sensitive to growth factors), leads to hypertrophy and proliferation of SMCs.
- Stress . Stress promotes activation of the sympathoadrenal system, which is accompanied by an increase in blood pressure and heart rate. In this case, parasympathetic influences on the heart are inhibited.
- Smoking . It has a stimulating effect on the sympathetic nervous system, disrupts endothelial function and activates endothelial vasoconstrictor factors.
- Metabolic syndrome – android obesity, insulin resistance, hyperinsulinemia, lipid metabolism disorders.
- Physical inactivity . Leads to a decrease in the adaptive capabilities of the most important systems of the body.
- Nutritional habits, excess body weight, high BMI.
- Increased sensitivity to Na intake. In this case, there is a retention of Na ions in the body, which causes an increase in blood pressure.
- Alcohol. Reduces the sensitivity of baroreceptors of the aorta and sinocarotid zone.
- Climatic factors . In some cases, hypertension can develop in young people after an average of 5 years of stay in the north.
- Gender and age. Women under 45 years of age have lower blood pressure levels than men. The increase in indicators in women occurs at the age of 40-59 years.
- Obstructive sleep apnea syndrome.
- Some industrial hazards (noise, vibration).
Pathogenesis
Normally, there are a number of pressor and depressor mechanisms that provide regulation of blood pressure.
Pressor:
- Short-term action (baroreceptor and chemoreceptor reflexes, SAS, CNS response to ischemia)
- Intermediate action (relaxation of tense vessels, changes in transcapillary exchange, RAS)
- Long-acting (aldosterone, vasopressin, renal-volume mechanism)
Depressor:
- Prostaglandins
- Kallikrekin-kinin
- Endothelial relaxing factor (NO)
- Atrial natriuretic peptide
Hemodynamic factors:
Blood pressure depends on the ratio of IOC, TPSS and BCC. Normally, these indicators are balanced and provide mutual compensation for each other. When the ratio of these indicators is violated, hypertension develops. There are several pathogenetic options:
- An increase in IOC, not accompanied by an adequate decrease in OPSS and BCC
- Increasing OPSS without adequately reducing IOC and BCC
- Simultaneous increase in IOC and OPSS
- An increase in blood volume associated with Na and water retention in the body
Neurogenic factors:
Eicosanoids: - PGF2α (prostaglandin F2α), - PGI2 (prostacyclin), PGE2, - EDHF - hyperpolarizing factor of endothelial origin (11,12-epoxyeicosatrienoic acid. - Endothelin - a group of peptides (I, II, III, ...) synthesized by endothelial cells. When angiotensin-II and/or vasopressin receptors bind endothelial cell membranes, they release endothelin-I into the interstitial space. Endothelin-I binds to the corresponding ETA receptors of the plasma membranes of adjacent smooth myocytes and triggers their contraction. Contraction of the muscle layer leads to constriction of the arteriole. Endothelin-I can bind to ETB receptors of endothelial cells and cause them to release nitric oxide, NO. Nitric oxide, acting on adjacent smooth myocytes, triggers their relaxation and dilation of the arteriole. – PO2, PCO2 - tension of oxygen and carbon dioxide in the interstitial environment. – NO – oxide concentration nitrogen in the interstitial environment. – K+, H+ - concentration of potassium ions, hydrogen ions in the interstitial environment. – ATP—concentration of adenosine triphosphate in the interstitial environment. – (M) - M-muscarinic receptors, cell membrane receptors for acetylcholine. – (H) - H-receptors of cell membranes for histamine. – (ETA), (ETA) - cell membrane receptors for endothelin-1. – ADH—vasopressin (antidiuretic hormone). – V1 - cell membrane receptors for vasopressin. – β2 - cell membrane receptors for adrenaline. In the nerve centers that regulate blood circulation, the number of pressor neurons is 4 times higher than depressor neurons. The depressor system is depleted much earlier than the pressor system, especially in conditions of depletion of the nervous system.
Activation of the sympathoadrenal system:
- An increase in heart rate leads to an increase in IOC
- Stimulation of alpha-adrenergic receptors leads to an increase in peripheral vascular resistance
- Vasoconstriction increases preload and IOC
Renin-angiotensin-aldosterone system:
Juxtaglomerular apparatus. Renin-angiotensin-aldosterone system. Renin is produced by the juxtaglomerular apparatus of the kidneys, in the blood it acts on →angiotensinogen synthesized by the liver, converting it into angiotensin1. Angiotensin1 becomes angiotensin2 under the action of angiotensin-converting enzyme. Also, angiotensinogen can be converted into angiotensin1 and angiotensin2 under the action of other enzymes - elastase, tissue plasminogen activator, cathepsin C. Angiotensin 2:
- Increases the tone of SMC vessels
- Facilitates impulse transmission in the sympathetic ganglia
- Stimulates the synthesis and release of aldosterone
- Stimulates the release and inhibits the reuptake of norepinephrine by nerve endings
- Stimulates the production of vasopressin and prostaglandin E2
- Increases blood volume
Endothelial dysfunction:
- The G-protein signaling system is disrupted
- NO secretion decreases
- Increased secretion of reactive oxygen species
- The reactivity of the endothelium to NO and endothelial depolarization factors decreases
2. Reasons
The most common congenital cause of renal hypertension is a fibromuscular malformation of the renal artery. Many other anomalies of the structure of the kidneys and renal vessels, bladder, ureters and urethra are also described as congenital causes.
Acquired causes include:
- atherosclerosis in the renal artery basin (statistically the most common cause);
- prolapse of the kidney (nephroptosis);
- an abnormal connection between the renal artery and vein, formed, for example, due to injury;
- arterial inflammation;
- mechanical pressure on the artery (by a growing tumor, cyst, hematoma, etc.).
It should be noted that the two most common causes, one congenital and one acquired (see above), together account for up to 98-99% of renovascular hypertension.
As for renin itself, its secretion and subsequent regulatory role represent a complex endocrine cascade, which involves protein precursor compounds, two forms of angiotensin, angiotensin-converting enzyme (ACE), and aldosterone (a hormone of the adrenal cortex). It is obvious that any failure in this multi-stage process, any damage or injury to secretory and/or receptor cells can cause endocrine imbalance and, accordingly, an excess of vasopressor hormones. Hypersecretion of renin may be a response to a purely mechanical reduction in the vasculature (blood supply) of the kidneys, however, the water-electrolyte balance is also grossly disturbed during inflammatory processes in the kidneys - glomerulo- and pyelonephritis, which leads to an excess volume of blood pumped by the heart and, as a consequence, to hypertension ( for example, bilateral pyelonephritis is accompanied by arterial hypertension in more than 40% of cases).
Visit our Cardiology page
Clinic
- Often asymptomatic and turns out to be an incidental finding during a visit to the doctor
- Frequent subjective manifestations are headaches in the occipito-parietal and temporal regions
- Cerebrovascular disorders are also possible - dizziness, tinnitus, spots before the eyes, decreased memory and mental activity
- Neurotic disorders - irritability, discomfort, fatigue, depression, sleep disturbance, uncertainty, anxiety
- 20-40% have cardiac pain syndrome
- Visual impairment
- Accent 2 tones over the aorta, hard pulse, tachycardia
- Changes in the boundaries of the heart, high apical impulse
3. Symptoms and diagnosis
There are some symptoms that are very characteristic of nephrogenic hypertension, but none of them are pathognomonic (characteristic of only one disease and not found in others). Thus, there are sharp and sudden increases in pressure against the background of normal heart rate, therapeutic resistance to conventional antihypertensive treatment (even intensive). However, in general, the symptoms can correspond to any form of arterial hypertension, so diagnosis in this case usually requires the involvement of several related specialists (cardiologist, vascular surgeon, endocrinologist, always an ophthalmologist, etc.). The primary task is to differentiate the renoparenchymal form of hypertension from the renovascular one. The anamnesis is carefully studied, examination, auscultation and percussion are performed, and a detailed and multifaceted laboratory examination is carried out. Of the instrumental diagnostic methods, the most informative are ultrasound, MSCT, various types of contrast urography and angiography (X-ray examination of blood vessels), kidney scintigraphy, radioimmunoassay of renin concentration in the blood, captopril test, etc. It should be noted that if a parenchymal form of renal hypertension is suspected, X-ray examinations should be prescribed with great caution and strictly according to indications, since both radiation exposure and X-ray contrast agents can aggravate damage to renal tissues and structures.
About our clinic Chistye Prudy metro station Medintercom page!
Classification
Stages of hypertension according to WHO 1962:
Stage I: BP>160/95 mm Hg. There are no target organ lesions. Stage II: BP>160/95 mm Hg. There are changes in target organs caused by hypertension. Stage III: BP>180/110 mm Hg. There are changes in target organs caused by hypertension with disruption of their function. Classification of blood pressure levels (WHO/MOAG, 1999)
In the national recommendations on hypertension (2010), risk factors, compared to previous ones, are no longer divided into basic and additional.
4.Treatment
As statistical analysis of the data accumulated in the world shows, conservative methods (medication, nutrition, etc.) are much less effective than active therapy and can only be used as auxiliary, preoperative, supportive measures, as well as palliative treatment in the presence of contraindications to surgical intervention. Surgical correction of renal arterial hypertension in most cases brings a lasting and pronounced positive result and significantly increases the life expectancy of such patients. Abdominal, endoscopic or percutaneous surgery is performed (depending on the clinical characteristics of a particular case) to restore the patency of stenotic arteries, eliminate congenital defects, or completely remove the affected and non-functioning kidney, which in some cases is the only effective answer. Approximately one third of patients may no longer take maintenance antihypertensive drugs.
Palliative antihypertensive therapy as an alternative to surgery, however, is also characterized by fairly high efficiency (although we can only talk about constant drug control of blood pressure) and allows one to normalize blood pressure to one degree or another in more than 90% of cases.