YES. Kuzhel, G.V. Matyushin, E.Yu. Egorova, N.V. Kovaleva
State Educational Institution of Higher Professional Education "Krasnoyarsk State Medical Academy"
KGBUZ "Krasnoyarsk Regional Hospital No. 2"
A test with dosed physical activity is an ideal method of functional diagnostics, which allows us to assess the usefulness of the physiological compensatory and adaptive mechanisms of the body, and in the presence of obvious or hidden pathology, the degree of functional inferiority of the cardiorespiratory system [1]. A stress test (ST) is considered one of the types of natural provocation, which is used to diagnose various diseases, and in cases where the pathology is already known, with the help of PT it is possible to determine the degree of its severity or the compensatory capabilities of the cardiovascular system. NP is one of several types of stress testing (along with transesophageal cardiac pacing, stress echocardiography), therefore the term NP more accurately reflects the essence of the technique than the often used definition of stress test.
The main point of application of the NP is the diagnosis of coronary artery disease. The most important advantages of NP are non-invasiveness, virtually unlimited availability and low cost of the study. The importance of NP is also emphasized by the fact that this technique allows us to identify a risk group, that is, patients at risk of developing cardiovascular complications and death. It is no coincidence that the recommendations for coronary angiography under class I indicate the following indication - “criteria for a high risk of cardiovascular complications identified by non-invasive testing, regardless of the severity of angina pectoris” [5]. However, the provocative nature of the test implies the possibility of various complications, many of which can be serious.
If non-dangerous complications are not taken into account, the incidence of fatal events during NP is relatively low. Thus, mortality during NP is estimated as one case per 50 thousand examinations. However, the incidence of non-fatal myocardial infarction and ventricular tachycardia remains quite high - one case per 2,500 studies, or 0.05% [6]. In this regard, it is important to note that complications of NP include events that occurred no later than 24 hours after the stress test [1, 4].
NP is usually performed using a treadmill or bicycle ergometer (VEM). Each method has certain advantages and disadvantages.
Treadmill (treadmill)
The treadmill must be electrically powered and capable of supporting a body weight of at least 157 kg [4]. The patient's movement during the treadmill test is forced, that is, the patient adapts to the speed of the treadmill, so any confusion during the load is fraught with injury. Taking this into account, for safety reasons it is recommended to equip the walkway with additional handrails on the sides of the device.
However, patients should avoid holding onto handrails if possible, as this reduces the amount of work being done due to some reduction in body weight. It may be recommended that patients hold handrails with their fingers to maintain body balance while walking, and an emergency stop button should be accessible to the patient and staff if necessary.
In most cases, the Bruce protocol (R. Bruce) is used to perform NP on the treadmill. In individuals with low exercise tolerance, a modified Bruce technique can be used. In this case, at the beginning of the test, steps with a less intense load are added (usually with a lower angle of elevation of the track at the same speed as in the first step of the Bruce protocol). At the same time, it must be especially emphasized that ideally the time of the NP itself should not exceed 9-12 minutes, therefore the protocol for both treadmill and VEM should be selected individually.
Indications for bicycle ergometry:
- detection of coronary artery disease (early and clinically pronounced forms);
- determination of exercise tolerance in patients with coronary artery disease and patients who have suffered a myocardial infarction;
- selection of medications, monitoring the effectiveness of treatment;
- detection of rhythm disturbances;
Bicycle ergometry is indicated not only for patients suffering from cardiovascular diseases, but also for healthy people:
- determination of the training regime for people exercising on exercise machines at home;
- persons of military age (VEM is a mandatory study during the military medical commission).
“SM-Clinic” is equipped with modern equipment for conducting stress tests, as well as other techniques used for diagnosing heart diseases.
VEM
VEM.
VEM may be considered as an alternative to the treadmill test in patients with orthopedic, vascular or neurological diseases. In addition, VEM is a less expensive and more portable system for performing NP. The intensity of work performed on the VEM can be adjusted by changing the pedaling frequency and resistance. The highest O2 consumption and heart rate values are usually achieved at a pedaling speed of 50-80 rpm. For NP, two types of stationary VEMs are used: with a mechanical or electric brake.
Mechanical ergometers require the patient to strictly follow the specified cadence in order to keep the amount of work performed constant. VEMs with electric brakes are more expensive and less portable, but automatically adjust resistance as cadence changes, thus keeping the work done constant. When performing HEM, the power of the first stage is usually 25 W (150 kgm/min) or 50 W (300 kgm/min) with a subsequent increase in load by 25 W until the final result is achieved. For individuals with high load tolerance, the load can be increased by adding 50 W.
In assessing the information content of any diagnostic test, the main criteria are its sensitivity and specificity, which determine how effectively the test separates subjects with pathology from healthy individuals, that is, how well the test allows diagnosing the disease and its absence. A meta-analysis of 147 published studies, including 24,074 patients who underwent both coronary angiography and NP, showed wide variability in sensitivity and specificity with averages of 68% plus/minus 16% and 77% plus/minus 17%, respectively [3]. it is believed that treadmill and VEM have the same sensitivity and specificity.
For the clinician, the most important information is to assess the likelihood of the presence or absence of the disease. Such an estimate cannot be accurately derived from the ST segment depression score alone, so an estimate of pretest disease probability is also required to more accurately interpret NP results. Based on this, the interpretation of NP results, according to Bayes' theorem, assumes that the probability of a disease after performing a test (TP) will be a derivative of its pre-test probability.
The clinician often makes this assessment intuitively, for example when suggesting a false-positive finding of ST segment depression in a 30-year-old woman with cardialgia. Therefore, given the relatively low specificity of ST segment depression greater than/equal to 1 mm in the diagnosis of IHD, this indicator cannot be considered as an absolute criterion of the disease, but should be assessed in the context of the pre-test probability of the disease.
The pre-test probability of coronary artery disease is assessed based on medical history, age, gender and the nature of pain in the chest, as well as an objective examination and instrumental studies. Typical or definite angina makes the pretest probability of the disease so high (more than 90%) that the need for an NP to diagnose coronary artery disease virtually disappears, but the test can be performed for risk stratification purposes.
Taking into account the high prevalence of the use of both the treadmill test and VEM in healthcare institutions, we conducted a comparative assessment of the effectiveness of these methods in the diagnosis of coronary artery disease.
Material and methods
The study was carried out on 107 patients on a treadmill (average age was 52.5 years, men - 74.6% and women - 25.4%) and 108 patients on VEM (average age was 49.4 years, men - 76.8% and women – 23.2%). NP on the treadmill was carried out according to the protocol of Bruce and mod. Bruce, NP on VEM was carried out according to the 50+25 and 25+25 protocol. The ECG was monitored in 12 standard leads, blood pressure was monitored at baseline, at the 2nd minute of each load step and at every minute of the recovery period. Upon completion of the load as a result of achieving a submaximal heart rate without electrocardiographic and clinical signs of angina, the test was regarded as negative.
If atypical discomfort in the chest appeared during exercise without ECG signs of myocardial ischemia, as well as ST segment depression of 1 mm or more in people with a low pre-test probability of coronary artery disease, the test was regarded as doubtful. A test terminated as a result of fatigue when submaximal heart rate was not achieved in the absence of clinical and ECG signs of myocardial ischemia was considered incomplete. Horizontal or other ST segment depression of 1 mm or more in individuals with an average or high pre-test probability of CAD was considered a positive test. The results of the study are presented in the table .
Discussion
The clinician, and with him the patient, are usually interested in two questions before performing NP. First, is there coronary atherosclerosis? The answer to this question seems quite ambiguous and may be misinterpreted, since the NP can confidently diagnose only hemodynamically significant occlusion of the coronary arteries. Secondly, is there a need for intervention [2]. Based on this, risk assessment or prognostic stratification is one of the turning points in medical practice.
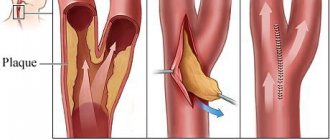
Most studies using NP have focused on the relationship between stress test scores and survival, whereas the relationship between NP scores and the risk of myocardial infarction is less clear. This is due to the fact that in most cases, significant cardiac events (sudden death, acute myocardial infarction and unstable angina) are caused by microscopic ruptures or damage to the atherosclerotic plaque. However, most vulnerable plaques appear to be angiographically insignificant before rupture (ie, with stenosis of less than 75% of the vessel diameter) and therefore may not produce clinical manifestations during loading. On the other hand, most significant plaques (those with greater than 75% stenosis) are stable on coronary angiography and have a low risk of rupture. Thus, the ability of any type of NP to detect vulnerable atherosclerotic plaques may be limited by the small size and reduced impact on coronary blood flow of these plaques, which may explain the acute coronary events that may occur soon after a negative stress test.
As can be seen from the results of our study (table)
The treadmill test was more sensitive in diagnosing IHD compared to VEM. A positive test was detected in 24.1% of patients on the treadmill and only in 9.6% on VEM. Of course, the results obtained, due to the small sample and, therefore, possible population differences, are of an evaluative nature and do not claim to be universal. However, it is possible that the more familiar, physiological nature of the treadmill load led to a greater number of completed trials, that is, studies reaching endpoints (submaximal heart rate, clinical angina, significant ST segment depression). On the other hand, VEM was accompanied by more frequent cases of incomplete tests, that is, termination of the test due to local fatigue of the muscles of the lower extremities before the development of clinical manifestations of the disease.
It is also noteworthy that VEM and treadmill test were relatively effective in identifying patients with angina pectoris of functional class III-IV, while the number of people with angina pectoris of functional class I-II diagnosed on a treadmill was significantly larger. Identification of patients with angina pectoris of medium and heavy loads is all the more valuable because it allows one to influence the process of coronary atherosclerosis through therapy at earlier stages, and also makes it possible to dynamically monitor patients and, therefore, control the disease process.
Table
Physiological basis of tests with gradually increasing cardiovascular load
Cardiovascular response
At the first stages of the stress test (up to 50% of the maximum load), cardiac output increases due to an increase in both heart rate and stroke volume; at a higher intensity of the load, the increase in cardiac output is caused mainly by an increase in heart rate; this adaptation mechanism allows, during maximum stress, to increase cardiac output by 4-6 times.
Physiological response to gradually increasing load
| Index | Designation and unit of measurement | English designation | Peace | Peak load | Increase compared to rest |
| Heart rate | Heart rate (bpm) | HR (bpm) | 70 | 180 | 2,6 |
| Stroke volume | VO (ml) | SV(mL) | 80 | 140 | 1,7 |
| Cardiac output | SV (l/min) | CO (L/min) | 5,6 | 25 | 4,5 |
| Systolic blood pressure | SBP (mmHg) | SBP (mmHg) | 120 | 180 | 1,5 |
| Diastolic blood pressure | DBP (mmHg) | DBP (mmHg) | 80 | 80 | 1 |
| Average blood pressure | BP avg. (mmHg.) | MAP (mmHg) | 93 | 113 | 1,2 |
| Total peripheral vascular resistance | OPSS (mm Hg/l/min) | TPR (mmHg/L/min) | 16,6 | 4,5 | 0,27 |
| Arteriovenous difference in O2 | Δ(a-c)O2 (ml/dl) | Δa-vO2 (mL/dL) | 5 | 16 | 3,2 |
| O2 consumption | PO2 (ml/min) | VO2 (mL/min) | 280 | 4000 | 14,3 |
| Breath volume | OD (ml) | Vt (mL) | 500 | 1800 | 3,6 |
| Breathing rate | RR (breaths/min) | BF (breaths/min) | 12 | 40 | 3,3 |
| Minute breathing volume | MOD (l/min) | VE (L/min) | 6 | 72 | 12 |
Systolic and mean blood pressure increase in parallel with the gradual increase in load, while diastolic blood pressure does not change or even decreases. In addition, a redistribution of blood flow occurs due to selective vasoconstriction of the mesenteric and other visceral arteries and vasodilation of the arteries of skeletal muscles involved in physical activity; Systemic vascular resistance is significantly reduced at both submaximal and maximum load levels. Resting heart rate, as well as its increase in response to increasing physical activity (i.e., chronotropic capacity) have a clear prognostic significance in asymptomatic patients: according to the results of the Framingham study, resting heart rate was associated with the level of total, cardiovascular and coronary mortality in 5070 asymptomatic men and women over a 30-year follow-up period. The correlation was stronger in men than in women and was independent of the presence of other cardiovascular risk factors. The risk of sudden cardiac death was closely related to resting heart rate. A smaller cohort study, the Framingham Offspring Study, examined the clinical significance of heart rate response to stepwise exercise. In this study, failure to achieve target heart rate (85% maximum for age), less increase in heart rate in response to exercise, and the chronotropic response index were predictors of all-cause mortality and morbidity of coronary artery disease. Not only the load-induced increase in heart rate, but also the process of heart rate recovery immediately after physical activity is closely related to the initial level of training and the state of the cardiovascular system. Cole et al. 2428 people with no history of coronary artery disease were observed for 6 years. Study participants performed a symptom-limited exercise test; heart rate recovery was defined as a decrease in maximum heart rate during the first minute after cessation of exercise; a decrease of less than 13 beats per minute was considered pathological. Insufficient heart rate recovery was a predictor of death (relative risk 4.0, CI 3.0–5.2), even after adjustment for sex, age, drug therapy, standard cardiovascular risk factors, and resting heart rate. The close relationship between the increase in heart rate in response to exercise and the recovery of heart rate after cessation of exercise and cardiovascular mortality highlights the clinical importance of routine exercise testing in assessing patient prognosis.
Respiratory response
The respiratory response to exercise can be accurately assessed during cardiopulmonary exercise testing, in which minute ventilation and expired gases (O2in and CO2ex) are measured while breathing through a face mask connected through an air flow transducer to a gas analyzer. Due to the technical complexity of the study, the cardiopulmonary stress test is not used for routine assessment of physical performance, however, it allows one to obtain important additional information for understanding the physiology of the pathological process in special categories of patients: with CHF, diseases of the respiratory system, candidates for transplantation, patients with decreased exercise tolerance for unclear reasons. The table provides a short list of the main abbreviations and technical terms used when performing cardiopulmonary exercise testing.
Abbreviations used when performing a cardiopulmonary test and interpreting its results
| Index | Designation and unit of measurement | English designation |
| Minute breathing volume | MOD (l/min) | VE (L/min) |
| Oxygen consumption per 1 min | O2vd (l/min) | VO2(L/min) |
| Carbon dioxide release in 1 minute | CO2out (l/min) | VCO2(L/min) |
| Oxygen partial pressure | PO2(mmHg) | PO2 (mmHg) |
| Partial pressure of carbon dioxide | PCO2 (mmHg) | PСO2 (mmHg) |
| Tidal volume (breathing volume) | OD (l) | VT(L) |
| Dead space volume | MP (l) | VD(L) |
| Functional residual capacity | FFU (l) | EELV(L) |
| O2 partial tension at end tidal expiration | PoutO2 (mm Hg) | PETO2(mmHg) |
| Partial pressure of CO2 at the end of quiet expiration | PoutCO2 (mmHg) | PETCO2(mmHg) |
| Ventilatory anaerobic threshold (if calculated per unit of body weight - ml/min×kg) | VAP (ml/min) | VAT (mL/min) |
| Peak oxygen consumption, measured at peak load individually for each patient, characterizes maximum performance (if calculated per unit body weight - ml/min×kg) | AUC (ml/min) | Peak VO2(mL/min) |
The respiratory response during the test with a gradually increasing load increases in proportion to the CO2 formed in the process of energy metabolism, which is necessary for its adequate removal from the body. Excess CO2, which is formed when lactate is buffered above the anaerobic threshold, leads to irritation of the respiratory center, as a result of which the minute volume of respiration (MVT) increases, which helps to maintain a linear relationship between MVT and produced CO2 (CO2 exhaled), resulting in the partial pressure of CO2 at the end of expiration ( PexCO2) remains unchanged. However, at the end of the stress test, hyperventilation also develops in relation to CO2 - as a respiratory compensation of load-induced metabolic acidosis, which leads to an increase in the ventilatory equivalent of CO2 (MOD/CO2out) and a decrease in PoutCO2. The ventilatory requirement to remove CO2 formed during metabolism is described by the modified alveolar equation:
MOD = (863 × CO2ext) / (PexCO2× [1 - MP/DO]),
where MP/DO is the ratio of physiological dead space (MD) to tidal volume (TV).
Metabolism in skeletal muscle
During gradually increasing physical activity, a level of energy demand is reached, above which the concentration of lactate in the blood plasma begins to rapidly increase (“anaerobic threshold”). This is a consequence of the activation of anaerobic glycolysis, which occurs under conditions where the rate of oxygen delivery is insufficient for the rapid oxidation of nicotinamide adenine dinucleotide (NADH) in the cytoplasm. Almost all H+ ions formed in cells from lactic acid (La) are neutralized by the bicarbonate buffer system:
H+ + La- + HCO3- ↔ H2O + CO2 + La-
Anaerobic metabolism is accompanied by excessive production of CO2 (excess CO2), this leads to the fact that the slope of the graph reflecting the dynamics of the ratio of CO2out to O2in becomes steeper. By measuring changes in the composition of exhaled gas caused by metabolic disorders, it is possible to determine the “ventilatory anaerobic threshold” by analyzing the ratio of CO2out to O2in. The ventilatory anaerobic threshold is the transition point from exclusively aerobic metabolism, when CO2ext / O2in ‹1, to aerobic-anaerobic metabolism, when CO2ext / O2in>1. In healthy people and cardiac patients without CHF, the ventilatory anaerobic threshold is usually at the level of 50-60% of peak O2 consumption, and in patients with CHF this figure increases.
Calculation of the respiratory anaerobic threshold: By measuring changes in the composition of exhaled gas caused by metabolic disorders, the “ventilatory anaerobic threshold” (VAT) can be determined by analyzing the ratio of CO2exhaled to O2inhaled (respiratory gas exchange coefficient). The ventilatory anaerobic threshold is the transition point from exclusively aerobic metabolism, when CO2exO2in ‹1, to aerobic-anaerobic metabolism, when CO2ex/O2in>1.
Criteria for achieving maximum load level
Achieving the maximum level of tension during a test with a gradually increasing load is a key point for assessing both the functional status and prognosis of patients; it can be determined by the following criteria:
- insufficient increase in O2bp and/or heart rate, its inconsistency with the increasing amount of work
- peak respiratory gas exchange coefficient (CO2ex/O2in) ≥1.10-1.15
- blood lactate concentration after exercise ≥8 mmol/dl (used in athletes, rarely achieved in patients)
- self-assessment of effort ≥8 (on a 10-point Borg scale)
- the patient's appearance (exhaustion).
Borg Physical Exercise Severity Rating Scale (Borg)
| Point | Interpretation |
| 0 | No load |
| 0,5 | Extremely light |
| 1 | Very light |
| 2 | Lightweight |
| 3 | Moderate |
| 4 | A little heavy |
| 5 | Heavy |
| 6 | |
| 7 | Very heavy |
| 8 | |
| 9 | |
| 10 | Extremely heavy |
| • | Maximum |
However, it must be remembered that all indicators of physical performance are only close to the actual maximum load level. In most cardiac patients, it becomes necessary to stop the stress test before achieving the listed criteria due to the development of cardiac symptoms (i.e., a symptom-limited stress test is performed). Peak physical performance, measured for example by maximal oxygen consumption, depends on three key physiological systems:
- efficiency of gas exchange in the lungs
- maximum cardiac output
- aerobic metabolic capacity of working skeletal muscles
Comparative results of the effectiveness of the treadmill test and bicycle ergometry
| Research result | Treadmill test number of patients /% | VEM number of patients /% |
| I. Negative test | 47 / 43,9% | 61 / 56,5% |
| II. Doubtful sample | 21 / 19,6% | 9 / 8,3% |
| III. Unfinished sample | 13 / 12,2% | 28 / 25,9% |
| IV. Positive test | 26 / 24,3% | 10 / 9,3% |
| 1. Low tolerance (III-IV FC) | 5 | 6 |
| 2. Average tolerance (II FC) | 20 | 4 |
| 3. High tolerance (I FC) | 1 | 0 |
Given the limitations of analyzing only ST segment depression in risk stratification, a number of authors have proposed using other indicators obtained during NP in prognostic assessment. Thus, using regression analysis, Mark et al [3] created the Duke score scale.
Duke scale
The Duke scale is calculated as follows: NP time according to the Bruce protocol (or MET) – 5 * (degree of maximum deviation of the ST segment in mm) – 4 * (angina index during NP). The angina index has a value of 0 if angina was not observed during NP, 1 if angina was recorded and 2 if angina was the reason for cessation of NP. If the ST segment deviation was less than 1 mm, the value entered into the ST deviation score was 0. Based on this scoring scale, a high-risk group was defined as having a score greater than/equal to -11 (average annual cardiovascular mortality greater than 5% ), as well as a group of low-risk patients – greater than/equal to +5 points (average annual cardiovascular mortality 0.5%).
Based on the data obtained, patients at high risk according to the Duke scale should be offered coronary angiography and, possibly, revascularization procedures [2]. Low-risk patients do not require additional examination and can receive conservative therapy. Patients at intermediate risk should undergo stress echocardiography as a test for further risk stratification. Patients with intermediate risk, dyssynergia of no more than one segment on stress echocardiography and normal heart size have a low risk of death and can receive conservative therapy. On the other hand, patients with the development of local contractility disorders of two or more segments on stress echocardiography should be referred to coronary angiography [2, 3].
Preparing for load testing
Before the examination, shave the skin of the chest in the area of the electrodes. The patient should eat his last meal 3 hours before the ECG (diabetics should take it with them). However, you must take drinking water with you. Subject should abstain from smoking for 4 hours. Drinking alcohol is prohibited the day before the test and on the day of the stress ECG. The test is best carried out in comfortable clothes and shoes.
You should not come for an examination at the last moment; it is better to set aside half an hour to have time to rest.