Chronic cerebrovascular accident (cerebral vascular insufficiency) is characterized by a decrease in blood supply to the brain. This condition is very common among older people in developed countries due to the high prevalence of atherosclerosis. In most cases, the carotid artery is damaged. A pair of carotid arteries, one on each side of the neck, running parallel to the jugular vein, are the main arteries that supply blood to the brain.
As a rule, cerebral vascular insufficiency develops in the area of the bifurcation of the carotid artery - the splitting of the carotid artery into internal and external branches. This splitting is similar to a stream that has split into two streams. In bifurcation, as well as during bifurcation in a water flow, accumulation of slag occurs. Severe symptoms begin to appear in most cases only when the artery blockage reaches 90 percent. This situation is similar to what happens with coronary heart disease.
Symptoms of chronic cerebrovascular accident are caused by decreased blood flow and oxygen supply to the brain. Stopping the flow of blood and oxygen leads to a stroke. The official definition of stroke is "loss of nerve function for at least 24 hours due to lack of oxygen." Some strokes are mild; others result in paralysis, coma, or speech impairment, depending on what part of the brain is involved. Mini-strokes, or transient ischemic attacks, can result in loss of nerve function for an hour or more, but less than 24 hours. TIAs can lead to transient symptoms of cerebral vascular insufficiency: dizziness, ringing in the ears, blurred vision, confusion, and so on.
Atherosclerosis is one of the main causes of cerebrovascular insufficiency. As this process progresses, high cholesterol levels combined with inflammation in the walls of the arteries in the brain can cause cholesterol to accumulate on the vessel wall in the form of a thick, waxy plaque. This plaque can restrict or completely prevent blood flow to the brain, causing stroke, transient ischemic attacks, or dementia, which can lead to a variety of other health complications.
The most common forms of cerebrovascular disease of the brain are thrombosis (40% of cases) and cerebral embolism (30%), followed by cerebral hemorrhages (20%).
Another form of cerebrovascular disease includes aneurysms. In women with defective collagen, weak key arterial branch points result in ridges with a very thin endothelial covering that can easily rupture with minimal increase in blood pressure. It can also occur with poor capillaries caused by cholesterol deposition in tissues, especially in hypertensive patients with or without dyslipidemia. If bleeding occurs, the result is a hemorrhagic stroke in the form of subarachnoid hemorrhage, intracerebral hemorrhage, or both.
A drop in blood pressure during sleep can lead to a marked decrease in blood flow in narrowed blood vessels, causing ischemic stroke in the morning. Conversely, a sharp increase in blood pressure due to daytime agitation can lead to rupture of blood vessels, resulting in intracranial hemorrhage. Cerebrovascular disease primarily affects people who are elderly or have a history of diabetes, smoking, or coronary heart disease.
TREATMENT OF BRAIN CIRCULATION DISORDERS IS AVAILABLE IN THE BRANCHES:
Treatment of cerebral circulatory disorders in the Primorsky region
Address: St. Petersburg , Primorsky district, st. Repisheva, 13
Treatment of cerebral circulatory disorders in the Petrograd region
Address: St. Petersburg , Petrogradsky district, st. Lenina, 5
Treatment of cerebral circulatory disorders in Vsevolozhsk
Address: Vsevolozhsk , Oktyabrsky Prospekt, 96 A
Dizziness as a manifestation of visual pathologies
The organ of vision indirectly maintains balance. Therefore, visual disturbances can cause dizziness.
Eye pathologies accompanying the development of an attack:
- deviation of the visual axis (squint);
- nystagmus (involuntary movements of the eyeball);
- glaucoma;
- cataract;
- weakened vision;
- astigmatism;
- diplopia (double image).
Symptoms of cerebrovascular accident
The initial signs of cerebrovascular accident are disturbances in concentration, memory, anxiety, irritability, mood swings, increased sentimentality, and tearfulness. Dizziness, episodes of loss of consciousness, blurred vision, changes in facial expression, slurred speech, or paresis of limbs may occur. These symptoms always require careful attention and a full neurological examination.
Causes of cerebrovascular accidents.
More often, vascular diseases predominate in older people. After 60 years, the risk of cerebrovascular accidents increases significantly, and the risk is higher in men than in women. The reasons may be:
- atherosclerosis,
- diabetes
- hypertension
- overweight, obesity,
- smoking
- low physical activity
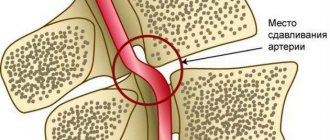
- Osteochondrosis of the cervical spine (compression of the arteries)
- heredity of vascular diseases
There are several types of cerebral blood supply disorders:
- acute cerebrovascular accident (stroke) - occurs suddenly.
- hemorrhagic (bleeding into the brain as a result of a ruptured vessel)
- acute ischemic circulatory disorder (ischemic stroke) – insufficiency of blood supply
- transient cerebrovascular accident - symptoms (loss of speech, blurred vision) last about a day, occur against the background of arterial hypertension or atherosclerosis.
- chronic cerebrovascular accident – develops gradually:
Stage 1 - drowsiness, fatigue, sleep disturbance, forgetfulness.
Stage 2 - memory impairment, motor dysfunction, depression, decreased performance, personality degradation.
Stage 3 - impairment of motor functions, speech, memory and dementia.
In case of cerebrovascular accident in children, the following is noted:
- increased fatigue
- weakness,
- headache
- disturbance of attention, memory and sleep
- Possible aggressiveness and short temper
Dizziness as a consequence of diseases of the internal organs
The appearance of such a symptom provokes the presence of diseases of the cardiovascular system or other organs in a person.
List of common pathologies whose symptoms include dizziness:
- abnormalities in heart rhythm;
- myocardial infarction;
- cardiomyopathy of various etiologies;
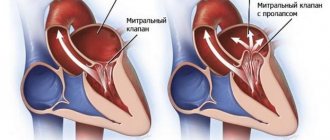
- dysfunction of the heart valves (heart defects);
- postural hypotension (a sharp drop in pressure when changing body position);
- excessive pulmonary ventilation due to nervous system disorders;
- anemia;
- diabetes;
- infection of the body;
- use of certain groups of drugs.
Diagnostics
An experienced neurologist can suspect and, in some cases, diagnose the condition based on the patient’s complaints. Additional examination methods help to identify the final cause:
- Dopplerography of the carotid artery (assessment of possible narrowing due to the atherosclerotic process).
- CT scan
- MRI
- EEG
- Clinical and biochemical blood test
! The earlier and more correctly the diagnosis is made, the more favorable the prognosis will be. !
Dizziness associated with pathologies
Such diagnoses include:
- Diseases of the inner ear: labyrinthitis, vestibular neuritis, etc. Such conditions lead to disturbances in the conduction of auditory and vestibular signals to the part of the brain that is responsible for recognizing these impulses.
- A cervical hernia compresses blood vessels, preventing proper blood circulation.
- Hypoxia due to stroke, thrombosis or ischemia.
- Migraine and attacks of benign paroxysmal vertigo.
- Brain tumors.
Treatment of cerebrovascular accidents
Treatment of cerebral circulatory disorders is usually aimed at improving blood flow, metabolic processes and protecting neurons from hypoxia (lack of oxygen). Treatment of cerebral circulatory disorders with cervical osteochondrosis and vascular disorders should be comprehensive and may include both traditional medicinal methods and various types of physiotherapy, manual therapy to get rid of the feeling of numbness in the arms or legs, and water procedures.
It should be understood that once this disease occurs, it “does not go away” and requires constant monitoring and adjustment of therapy, prevention of complications!
In our clinic you can undergo a full examination by qualified specialists in various fields.
Physiological dizziness
Not in all cases, dizziness is a manifestation of the disease. Sometimes this is how the body reacts to stimuli. This condition is provoked by:
- A rapid movement in which the body sharply deviates from the horizontal: riding on a swing, jumping from a height.
- Anxiety, panic attacks, fright, during which excess amounts of stress hormones are released into the blood.
- Oxygen starvation, which occurs due to a lack of iron in the blood or for other reasons.
- Hyperventilation of the lungs.
- Hypoglycemia is exhaustion of the body due to a lack of glucose.
- Dizziness as a sign of pregnancy. The monthly physiological state of a woman during the premenstrual period or during menstruation.
- Menopausal syndrome.
Cost of treatment of cerebral circulatory disorders:
| Services list | Price in rubles | |
| Saint Petersburg | Vsevolozhsk | |
| Initial appointment with a 1st level neurologist | 1850 | 1700 |
| Repeated appointment with a 1st level neurologist | 1650 | 1500 |
| Initial appointment with a 2nd stage neurologist | 2100 | — |
| Repeated appointment with a 2nd stage neurologist | 1900 | — |
| Initial appointment with neurologist Kolyada A.A. | 3200 | — |
| Repeated appointment with neurologist Kolyada A.A. | 2900 | — |
| Initial appointment with a neurologist Eroshina E.S./Irishina Yu.A./Tsinzerling N.V. | 4000 | 4000 |
| Repeated appointment with a neurologist Eroshina E.S./Irishina Yu.A./Tsinzerling N.V. | 3500 | 3500 |
| Initial appointment with neurosurgeon A.I. Kholyavin | 3300 | — |
| Repeated appointment with neurosurgeon A.I. Kholyavin | 2900 | — |
| Neurologist's report for reference | 700 | 700 |
| MANIPULATION | ||
| Piriformis muscle block | 2000 | 2000 |
| Occipital nerve block | 1800 | 1800 |
| Carpal tunnel block | 2500 | 2500 |
| Block of the sacroiliac joints | 2700 | 2700 |
| Suprascapular nerve block | 1800 | 1800 |
| Botulinum therapy | 5300 | 5300 |
| Botulinum therapy for bruxism and chronic facial pain | 18000 | — |
| Infusion relief of acute back pain syndrome | 1750 | 1750 |
| Plasmolifting (1 procedure) | 3100 | 2800 |
| Transcranial polarization in Parkinson's disease (30 min) | 1800 | — |
| Pharmacopuncture | from 1500 | from 1500 |
| HEADACHE TREATMENT | ||
| Botulinum therapy for chronic migraine | 35000 25900 | 35000 25900 |
| Targeted treatment of migraine (1 session) | 17900 | 17900 |
Diagnosis of dizziness
To get a diagnosis, see a doctor. The profile of the specialist has been discussed above. In such situations, health workers act by elimination, so you will need to do a number of studies:
- Ultrasound of the great vessels of the head and neck;
- examination by an ophthalmologist;
- ENT examination, audiogram if necessary;
- X-ray, CT or MRI of the spine and brain (the specific diagnostic procedure is recommended by the doctor);
- laboratory tests (tests).
Treatment is prescribed only based on the results of a comprehensive examination.
A condition in which dizziness is a common occurrence. You should not ignore the problem or tolerate it. Dizziness is not uncommon as a sign of serious health problems. Timely measures are the key to a successful resolution of the situation. If the examination does not reveal any organic pathologies, maintenance therapy will be prescribed.
Publications in the media
Dizziness is one of the most common symptoms in neurological and general somatic practice. Complaints of dizziness rank third after complaints of headache and back pain. First of all, you must remember that dizziness is just a symptom and not an independent disease. It can be a manifestation of various sufferings - cardiovascular, endocrine, mental, diseases of the spine, brain, etc., in total there are about 80 different nosological forms. Determining the causes of dizziness and its treatment require a multidisciplinary approach, and sometimes the use of complex equipment. Due to these objective difficulties, no more than 20% of patients receive a correct diagnosis and adequate treatment [1].
The head of a large otoneurological clinic in Germany and the author of the famous monograph “Dizziness,” Thomas Brandt, cites in it the most common causes of dizziness. Psychogenic dizziness, including paroxysmal phobic dizziness, ranks second after benign paroxysmal dizziness (Fig. 1).
The cause of psychogenic dizziness can be any mental illness, but most often anxiety disorders.
Diagnosis of psychogenic dizziness
Psychogenic dizziness refers to vague sensations described as dizziness, which most often occur in neurotic, stress-related disorders.
Diagnosis of psychogenic dizziness includes two sequential and mandatory stages.
The first stage is a negative diagnosis aimed at excluding all other possible causes of dizziness:
- damage to the vestibular system at any level;
- somatic and neurological diseases accompanied by lipothymia;
- neurological diseases accompanied by impaired walking and balance.
This requires a thorough examination of the patient, in some cases with the involvement of otoneurologists, cardiologists, hematologists, etc., as well as a thorough paraclinical study.
Thus, when examining a patient with dizziness at the first stage, it is important to determine the type of dizziness. To do this, you should carefully collect anamnesis - ask the patient in detail what he means by the word “dizziness.” With vestibular, systemic, true vertigo or vertigo, the patient experiences an illusory sensation of movement of a stationary environment in any plane, as well as a sensation of movement or rotation of his own body. The cause of systemic dizziness is damage to the vestibular analyzer at the peripheral or central level.
Psychogenic dizziness is always non-systemic in nature. The patient describes any sensations other than rotation: fog in the head, instability, fear of falling, and others.
When making a differential diagnosis, it is also extremely important to identify and clarify the nature of concomitant somatic and neurological manifestations to exclude other “organic” causes of non-systemic dizziness. For this purpose, a study of nystagmus, balance tests, audiography, computed tomography (CT) or magnetic resonance imaging (MRI), Doppler ultrasound of the main arteries of the head, compression-functional tests, radiography of the skull, internal auditory canal, cervical spine, complete blood count, fasting blood sugar, blood urea nitrogen and other studies [4].
The second stage is a positive diagnosis of neurotic disorders associated with stress.
Among emotional disorders, the most common cause of dizziness is anxiety or anxiety-depressive disorders. It is the frequency of anxiety, which is the most common emotional disorder and is observed in 30% of the population, that determines the high prevalence of psychogenic dizziness.
The clinical picture of anxiety disorders consists of mental symptoms, the most common of which are anxiety, worry about trifles, a feeling of tension and stiffness, as well as somatic symptoms, mainly caused by increased activity of the sympathetic division of the autonomic nervous system. One of the commonly observed physical symptoms of anxiety is dizziness and lightheadedness. The combination of mental and physical symptoms is not accidental - when the body is threatened or there is any potential threat, preparation occurs to fight the danger or flee from it. These changes in the body are ensured by the autonomic nervous system, which is a potential “bridge between the psyche and soma.” The most common symptoms of anxiety are presented in Fig. 2, 3.
Purely anxiety disorders are relatively rare in clinical practice. In most cases, in 70% of patients, anxiety disorders are combined with depressive disorders. The mental symptoms of anxiety and depression are largely similar and overlap. The comorbidity of the two most common mental disorders is determined by common biochemical roots—the role of serotonin in the pathogenesis of both conditions is discussed. The high effectiveness of both tricyclic antidepressants (TCAs) and some selective serotonin reuptake inhibitors (SSRIs) for both anxiety and depression confirms that serotonin has both anxiolytic and antidepressant effects. Finally, with the long-term existence of anxiety disorders, the patient inevitably develops a feeling of complete spiritual paralysis and depression develops. The onset of depression is accompanied by symptoms such as chronic pain disorder, weight loss, sleep disturbances, and others, which can increase symptoms of anxiety. Thus, a vicious circle develops: the prolonged existence of anxiety causes the development of depression, and depression increases the symptoms of anxiety. The high frequency of comorbidity of anxiety and depression is taken into account in the latest classifications - a special subgroup has been identified within anxiety states - mixed anxiety-depressive disorder.
According to ICD-10, there are four types of anxiety disorders: anxiety disorders (generalized anxiety disorder, mixed anxiety-depressive disorder, panic disorder); phobic anxiety states (simple phobias, social phobia, agoraphobia); obsessive-compulsive disorder; reactions to a stressful stimulus (simple reactive disorder, post-stress reactive anxiety disorder).
The feeling of dizziness most often occurs in patients with generalized anxiety disorder. In this case, the patient suffers from constant unjustified or exaggerated fears for his family, health, work or material well-being. At the same time, an anxiety disorder is formed regardless of any specific life event and, thus, is not reactive. In such a patient, at least six of the common anxiety symptoms listed above may be observed every or almost every day for more than six months—the “rule of six.”
A patient with generalized anxiety, when visiting a neurologist, rarely reports mental symptoms, but, as a rule, presents a lot of somatic (vegetative) complaints, where dizziness can be the leading symptom, or actively presents the only complaint of dizziness. This happens because the patient is most alarmed by the feeling of dizziness, thoughts of a stroke or other serious brain disease arise, mental disorders - fear, impaired concentration, irritability, wariness, etc. are regarded as a reaction to severe, currently not identified illness. In other cases, mental disorders are mild, and the clinical picture is actually dominated by dizziness. The latter option is especially common in cases where anxiety disorders occur in patients with congenital vestibulopathy. Such people have an imperfect vestibular apparatus since childhood. This is manifested in their poor tolerance to transport (sickness), poor tolerance to heights, swings and carousels. In an adult, these symptoms are less relevant; over the years, the vestibular apparatus is trained and vestibular disorders are compensated, however, when anxiety occurs, various sensations may arise - instability, fog in the head, etc., which are interpreted by them as dizziness.
One of the most important features of psychogenic dizziness is its combination with disorders in other systems, since the somatic manifestations of anxiety are always multisystemic (
). The ability of a doctor to see, in addition to complaints of dizziness, the disorders that naturally accompany it in other systems, allows us to understand its clinical essence and determine its psychosomatic (vegetative) nature [7]. For example, dizziness in generalized anxiety disorder is often associated with increased breathing (hyperventilation syndrome), in which, due to excessive blood oxygen saturation and hypocapnia, presyncope, paresthesia, muscle spasms or cramps, cardialgia associated with increased tone of the pectoral muscles may develop. as a result of increased neuromuscular excitability, tachycardia, etc. To identify polysystemicity, it is necessary to actively ask the patient about the presence of other complaints and disorders in addition to dizziness.
Psychogenic dizziness can also be one of the main symptoms of panic disorder. It is characterized by the recurrence of panic attacks and anxiety in anticipation of the next attack. The diagnosis of a panic attack is characterized by the presence of emotional disorders, the severity of which can range from a feeling of discomfort to panic and other mental or somatic symptoms - at least 4 out of 13, among which one of the most common is dizziness. Dizziness in the picture of a panic attack can occur spontaneously, without any apparent reason, in the words of patients - “out of the blue.” However, in more than half of the cases, it is possible to find out that dizziness arose after emotional stress or fear experienced by the patient, especially for the very first and, as a rule, the most severe attack.
A special type of phobia is phobic postural vertigo. It is described by patients as instability in the form of attacks (seconds or minutes) or a feeling of an illusory violation of the body’s stability lasting a fraction of a second and can occur spontaneously, but is more often associated with special perceptual stimuli (overcoming a bridge, stairs, empty space) [2].
The most demonstrative is psychogenic dizziness in patients suffering from agoraphobia. At home, surrounded by relatives or a medical facility, the patient may not experience dizziness or it may be mild (serve himself, do housework without difficulty). A neurological examination does not reveal any walking or balance disorders in such a patient when special tests are carried out. When moving away from home, especially in transport, in the subway, dizziness, gait disturbance, instability, suffocation, heart pain, tachycardia, nausea, etc. occur.
In all of these cases, dizziness is a symptom, a manifestation of one or another type of anxiety disorder.
Thus, the following clinical features of psychogenic dizziness can be distinguished:
- Dizziness is intermittent and has been described as “brain fog,” a feeling of mild intoxication, or a fear of falling. Fluctuating instability in the form of attacks (seconds or minutes) or a sensation of an illusory violation of the body’s stability lasting a fraction of a second is possible.
- Dizziness appears spontaneously, but is often associated with specific perceptual stimuli (bridge, stairs, empty space) or situations that are perceived by the patient as provoking factors (subway, department store, meeting, etc.).
- Dizziness and complaints occur in a standing position and while walking, despite the normal performance of stability tests such as the Romberg test, tandem walking, standing on one leg, etc. With psychogenic dizziness, a significant decrease in staggering in the Romberg position is often noted when distraction - psychogenic Romberg.
- The cardinal clinical sign of psychogenic dizziness is its combination with disorders in other systems (polysystemic), which indicates its secondary psychosomatic (vegetative) nature.
- The onset of the disease follows a period of fear or emotional stress and often occurs in individuals with vestibulopathy (congenital deficiency of the vestibular apparatus).
- Anxiety and anxiety-depressive disorders accompany dizziness, although dizziness can occur without anxiety.
- There are no objective clinical and paraclinical signs of organic pathology.
Psychogenic dizziness occurring after benign paroxysmal vertigo
Benign paroxysmal vertigo (BPV) is the most common type of vertigo. Its cause is cupulolithiasis - the formation of deposits (detritus) in the semicircular canals of the inner ear, which irritate the receptors as they move and cause severe vestibular vertigo. When changing body position, often when getting out of bed or turning the head, the patient experiences a feeling of strong rotation, lasting from several seconds to a minute and accompanied by nausea, vomiting and other vegetative symptoms. To diagnose BPH, the Hallpike test is used. The patient turns his head 30 degrees to the side and moves from a vertical to a horizontal position with his head slightly tilted back. At the same time, he experiences severe systemic dizziness and nystagmus. The disease is benign, but is prone to relapse. To treat it, special Epley positional techniques are used, the task of which is to mechanically remove detritus from the posterior semicircular canal of the inner ear, after which the dizziness stops.
An attack of BPH is always difficult for the patient, can be repeated when turning the head, chains him to bed, and forces him to take a forced position. Undoubtedly, DPG is a stress-generating factor, is accompanied by fear and can provoke reactive anxiety disorder in an emotionally labile person. In some cases, the anxiety disorder that develops following DPG is iatrogenic. Doctors often misdiagnose patients with BPH as acute cerebral circulatory disorders in the vertebrobasilar system, hospitalize them, and conduct massive courses of vascular therapy, thereby convincing the patient of the severity of his condition and the presence of a fatal disease. In such frequent cases, the patient develops an anxiety disorder as a reaction to a severe neurological disease. Dizziness becomes unsystematic (instability, fear of falling, fog in the head, etc.), acquires a constant course, periodically intensifying. In such cases, both negative and positive diagnosis of psychogenic dizziness are especially important. A Hallpike test is mandatory. It must also be remembered that acute cerebrovascular accidents (ACVA) in the vertebrobasilar system, in addition to dizziness, are necessarily accompanied by other signs of damage to the brain stem: oculomotor, bulbar, sensory and other disorders.
Treatment of psychogenic dizziness
In the treatment of psychogenic dizziness, complex therapy is used, combining both non-drug and medicinal treatment methods [7].
Non-drug treatments include:
1) vestibular gymnastics, aimed at training and reducing the excitability of the vestibular apparatus; 2) breathing exercises: transition to the abdominal type of breathing, in which exhalation is twice as long as inhalation. Such breathing exercises reduce hyperventilation disorders comorbid with psychogenic dizziness. To relieve severe hyperventilation disorders, during a hyperventilation crisis, breathing into a paper or plastic bag can be recommended; 3) the most effective method of treatment is psychotherapy.
Medicinal methods.
1) Psychotropic therapy has priority in the treatment of psychogenic dizziness.
The first-line drugs for the treatment of anxiety disorders are antidepressants - SSRIs, Paxil and Fevarin have an anxiolytic effect; tricyclic antidepressants (amitriptyline) are used less frequently due to the presence of a large number of side effects and poorer tolerability. Traditional anxiolytics are benzadiazepines (Phenazepam, Diazepam, Alprazolam, Clonazepam, etc.). In some cases, a positive effect in the treatment of anxiety disorders is achieved with the use of “small” antipsychotics (sulpiride, tiapride, thioridazine), usually using small doses.
The drug Atarax (hydroxyzine) has shown pronounced effectiveness against psychogenic dizziness developing as part of generalized anxiety disorder. Atarax is an H1-histamine receptor blocker. It has a pronounced anti-anxiety, antihistamine, antipruritic and antiemetic effect. In a study conducted at our department, prof. Solovyova A.D., it was shown that in patients with vegetative dystonia syndrome, which is the main neurological manifestation of generalized anxiety disorder, complaints of dizziness and lipothymic (presyncope) states decreased by almost 80%.
2) Additional therapy.
As an additional therapy, the drug Betahistine is used, which reduces the excitability of the vestibular apparatus and is effective for all types of dizziness, including psychogenic.
The effectiveness of Betaserc was tested in patients with psychogenic dizziness using a special computer program developed by the staff of the Institute of Medical and Biological Problems, prof. Kornilova L.N. et al. In a joint study with our department [6], it was shown that the drug objectively improves vestibular reactivity and the state of the oculomotor system (
). A follow-up study revealed that the effectiveness of Betaserc was temporary, so it should be used for a long time for this type of dizziness as an additional therapy, especially in cases where dizziness develops in people with congenital vestibulopathy and acts as a leading somatic symptom.
E. G. Filatova, Doctor of Medical Sciences, Professor of the Federal Faculty of Applied Physics of Moscow Medical Academy named after. I. M. Sechenova
Treatment of dizziness
Diagnoses vary. And while some conditions can be treated conservatively, others require emergency or planned surgical intervention.
Conservative treatment is prescribed by a specialist who deals with the problem indicated by laboratory and instrumental studies.
Dizziness is not an independent diagnosis, but a manifestation of an underlying disease. Therefore, symptomatic and etiotropic treatment will be required, aimed at eliminating both the cause of the disease and its consequences. The first thing they do is try to influence the symptom that brought the patient to the walls of the medical facility: do everything to stop the dizziness. Then they delve into the original source, affecting the epicenter of the disease.
The doctor will select the necessary medications and procedures, and at the same time give recommendations on physical activity, nutrition, etc. Treatment methods are aimed not only at stabilizing the patient’s condition, but also at long-term prevention of relapses of dizziness attacks.
The effectiveness of treatment depends on the timeliness of diagnosis, the qualifications of the attending physician and the patient’s responsible attitude to the recommendations received. Take care of yourself and be healthy!