Diets and various dietary restrictions lead to disruption of the natural intake of various micro- and macroelements, vitamins, and minerals from food. To normalize the functioning of the body, it is necessary to balance not only the calorie content, carbohydrate and protein composition of food, but also include foods rich in various elements in the diet. One of the most important minerals for humans is phosphorus P: it accounts for about 1% of the total human mass. What is phosphorus responsible for and how to compensate for its deficiency with food?
The role of phosphorus in the human body
Daily intake of phosphorus
Phosphorus-rich foods
Why is it needed?
The main function of phosphorus is the formation of bones and teeth in “commonwealth” with calcium and fluorine.
For the construction of bone tissue they form the compound calcium hydroxyphosphate, and for dental tissue they form calcium fluorophosphate. The Dangers of Vegetarianism
Refusal of food of animal origin is fraught not only with phosphorus deficiency. Vegetarians over time become deficient in vitamins A1, B2, B12 and D, calcium, iron, zinc and essential polyunsaturated fatty acids. These substances are absent from plant foods or are very poorly absorbed from them.
Because phosphorus is a component of many enzymes, it plays an important role in the body's use of carbohydrates and fats and in protein synthesis for the growth and regeneration of cells and tissues. Phosphorus is used to produce ATP, molecules the body uses to store energy. This substance also helps the kidneys function properly, regulates muscle contractions (including cardiac ones) and improves the conductivity of nerve fibers.
Properly selected nutrition is the key to longevity and excellent well-being.
The role of food in our lives is not only to satisfy hunger, but also to fill the body with useful substances. For a good mood and good health, a person needs a large number of valuable elements.
Food should have pleasant organoleptic properties, create a long-lasting feeling of fullness, not be burdensome for the digestive system, and be easily digested. It must be harmless against microorganisms, toxic substances and radionuclides.
Macro and micronutrients are of great importance in human nutrition.
A balanced combination of macro and micronutrients in the diet is necessary for the healthy and long-term functioning of the complex human body.
Macronutrients are nutrients that a person needs every day and in large quantities (we're talking about hundreds of grams). They promote body growth and supply energy and nutrients.
These include proteins, fats, carbohydrates and water.
Micronutrients are nutrients required by the body in mini-doses (milligrams). Promote the absorption of energy, the proper development of the body and coordinate various tasks.
These include minerals and vitamins.
What if it's not enough?
A normal balanced diet is enough to fully satisfy the need for phosphorus. Those who do not consume animal products at all are at risk of experiencing a deficiency of the substance. Excess phosphorus is also dangerous. If a person has kidney disease, even a slight excess of the daily intake of the substance can be dangerous for him. In this case, you need to carefully monitor your phosphorus intake and not exceed a dose of 800 mg per day. This is necessary because the processes of calcium and phosphorus metabolism are related to each other. A severe increase in the amount of phosphorus in the body reduces calcium levels and leads to bone diseases.
Requirements for vitamins and minerals in children of different ages
In childhood neurodietology, the need for regular consumption of vitamins and minerals is an axiom [1]. It is these essential substances, related to micronutrients, that make it possible to ensure normal physical development and adequate functioning of all organs and systems of the body, including the central nervous system [2].
By analogy with vitamins, the inadequate consumption of which is accompanied by vitamin deficiency conditions or hypovitaminosis, insufficient intake of minerals into the body can lead to microelementosis (or diselementosis) in children and adults [3–5]. In particular, this applies to such minerals as magnesium (Mg), zinc (Zn) and calcium (Ca), each of which was previously discussed in our respective publications [6–11].
The question of the advisability of simultaneous or time-separated intake of vitamins and minerals continues to be debatable, but, apparently, this point cannot be considered fundamental. It is undeniable that children's needs for vitamins and minerals are strictly age-dependent.
The positive effect of subsidies of vitamins and minerals on the body of the unborn child can be stated when women take specialized complexes in a timely manner during pregnancy [12–14]. Previously, we have repeatedly reported on the so-called “vitamin lines” aimed at children of various ages [15–18]. This approach to providing children with vitamin and vitamin-mineral complexes at various stages of postnatal ontogenesis can already be considered traditional by the beginning of the 21st century. An example of such “lines” is the Supradin Kids line; these vitamins are registered in the Russian Federation as dietary supplements [19]. Representatives of the Supradin Kids line are characterized by the presence in their composition of biologically active substances (lecithin, choline, omega-3 fatty acids, β-carotene), aimed at modulating cognitive and neurological functions in children of different ages.
The “Norms for physiological needs for energy and nutrients for various groups of the population of the Russian Federation”, in force since 2008 in the Russian Federation, have revised and clarified children’s need for vitamins and minerals depending on age [20]. The previously presented “Norms of physiological needs for nutrients and energy for various groups of the population of the USSR” dated back to 1991.
When providing data on the needs for vitamins A (retinol) and E (tocopherol), the abbreviations “ret. eq." (retinol equivalent, 1 mcg ret. eq. corresponds to 1 mcg retinol) and “current. eq." (tocopherol equivalent, 1 mg current equivalent corresponds to 1 mg alpha-tocopherol).
For children of the first year, the norms for vitamin C consumption remained the same (0-3 months - 30 mg/day, 4-6 months - 35 mg/day, 7-12 months - 40 mg/day), vitamin A (0-12 months - 400 mcg ret. equiv./day), vitamin E (0–6 months — 3.0 mg current. eq./day), vitamin D (0–12 months — 10 mcg/day), vitamin B1 (0–3 month - 0.3 mg/day, 4-6 months - 0.4 mg/day, 7-12 months - 0.5 mg/day), vitamin B2 (0-3 months - 0.4 mg/day, 4 –6 months - 0.5 mg/day, 7-12 months - 0.6 mg/day), vitamin B6 (0-3 months - 0.4 mg/day, 4-6 months - 0.5 mg/day , 0.6 mg/day) and vitamin B12 (0–3 months — 0.3 mcg/day, 4–6 months — 0.4 mcg/day, 7–12 months — 0.5 mcg/day). In the updated recommendations, the need for vitamin PP (niacin) in children aged 7–12 months has increased to 7 mg/day (previously 4 mg/day), as well as the norms of dietary intake of folic acid (0–6 months - 50 mcg/day instead of 40 mcg/day). A previously missing recommendation for the consumption of vitamin B5 (pantothenic acid) has appeared: at the age of 0-3 months - 1.0 mg/day, 4-6 months - 1.5 mg/day, 7-12 months - 2.0 mg/day . Unfortunately, the need for vitamin K and biotin in children of the first year of life is not specified [20].
For children over 12 months of age, the following vitamin intake standards are currently recommended in Russia:
- ascorbic acid (1-3 years - 45 mg/day, 3-7 years - 50 mg/day, 7-11 years - 60 mg/day, 11-14 years - 70 mg/day for boys and 60 mg/day for girls, 14–18 years old - 90 mg/day for adolescents and 70 mg/day for girls);
- vitamin A (1-3 years - 450 mcg ret. eq./day, 3-7 years - 500 mcg ret. eq./day, 7-11 years - 700 mcg ret. eq./day, 11-18 years - 1000 mcg ret.eq./day for boys and 800 mcg ret.eq./day for girls);
- vitamin E (1-3 years - 4.0 mg current equivalent/day, 3-7 years - 7.0 mg current equivalent/day, 7-11 years - 10.0 mg current equivalent/day , 11-14 years old - 12.0 mg current equivalent/day, 14-18 years old - 15 mg current equivalent/day);
- vitamin D (1–18 years - 10 mcg/day);
- vitamin B1 (1-3 years - 0.8 mg/day, 3-7 years - 0.9 mg/day, 7-11 years - 1.1 mg/day, 11-14 years - 1.3 mg/day , 14–18 years old - 1.5 mg/day for boys and 1.3 mg/day for girls);
- vitamin B2 (1-3 years - 0.9 mg/day, 3-7 years - 1.0 mg/day, 7-11 years - 1.2 mg/day, 11-14 years - 1.5 mg/day , 14–18 years old - 1.8 mg/day for boys and 1.5 mg/day for girls);
- vitamin B6 (1-3 years - 0.9 mg/day, 3-7 years - 1.2 mg/day, 7-11 years - 1.5 mg/day, 11-14 years - 1.7 mg/day for boys and 1.6 mg/day for girls, 14–18 years old - 2.0 mg/day for boys and 1.6 mg/day for girls);
- vitamin B12 (1-3 years - 0.7 mcg/day, 3-7 years - 1.5 mcg/day, 7-11 years - 2.0 mcg/day, 11-14 years - 3.0 mcg/day );
- niacin (1-3 years - 8.0 mg/day, 3-7 years - 11.0 mg/day, 7-11 years - 15.0 mg/day, 11-14 years - 18.0 mg/day, 14–18 years old - 20.0 mg/day for boys and 18.0 mg/day for girls);
- biotin (1-3 years - 10.0 mcg/day, 3-7 years - 15.0 mcg/day, 7-11 years - 20.0 mcg/day, 11-14 years - 25 mcg/day, 14- 18 years old - 50 mcg/day);
- folic acid (1-3 years - 100 mcg/day, 3-11 years - 200 mcg/day, 11-14 years - 300-400 mcg/day, 14-18 years - 400 mcg/day);
- vitamin B5/pantothenic acid (1-3 years - 2.5 mg/day, 3-11 years - 3.0 mg/day, 11-14 years - 3.5 mg/day, 14-18 years - 5.0 mg/day for boys and 4.0 mg/day for girls);
- vitamin K (1-3 years - 30 mcg/day, 3-7 years - 55 mcg/day, 7-11 years - 60 mcg/day, 11-14 years - 80 mcg/day for boys and 70 mcg/day for girls, 14–18 years old - 120 mcg/day for boys and 100 mcg/day for girls) [20].
If until 2008, children’s consumption of only 6 mineral substances (Ca, P, Mg, Fe, Zn and I) was regulated, now there are recommendations for the consumption of 13 elements in childhood. Among them, in addition to those already listed, are potassium (K), sodium (Na), chlorine (Cl), copper (Cu), selenium (Se), chromium (Cr) and fluorine (F) [20].
It should be noted that there are no recommendations on the daily requirement for potassium (K) and chromium (Cr) for children in the first year of life.
Since 2008, the following standards for the consumption of mineral substances by children of different ages have been provided:
- calcium (0–3 months — 400 mg/day, 4–6 months — 500 mg/day, 7–12 months — 600 mg/day, 1–3 years — 800 mg/day, 3–7 years — 900 mg/day day, 7–11 years – 1100 mg/day, 11–18 years – 1200 mg/day);
- phosphorus (0–3 months — 300 mg/day, 4–6 months — 400 mg/day, 7–12 months — 500 mg/day, 1–3 years — 700 mg/day, 3–7 years — 800 mg/day day, 7–11 years – 1100 mg/day, 11–18 years – 1200 mg/day);
- magnesium (0–3 months — 55 mg/day, 4–6 months — 60 mg/day, 7–12 months — 70 mg/day, 1–3 years — 80 mg/day, 3–7 years — 200 mg/day day, 7–11 years – 250 mg/day, 11–14 years – 300 mg/day, 14–18 years – 400 mg/day);
- potassium (1-3 years - 400 mg/day, 3-7 years - 600 mg/day, 7-11 years - 900 mg/day, 11-14 years - 1500 mg/day, 14-18 years - 2500 mg/day day);
- sodium (0–3 months — 200 mg/day, 4–6 months — 280 mg/day, 7–12 months — 350 mg/day, 1–3 years — 500 mg/day, 3–7 years — 700 mg/day day, 7–11 years – 1000 mg/day, 11–14 years – 1100 mg/day, 14–18 years – 1300 mg/day);
- chlorides (0–3 months — 300 mg/day, 4–6 months — 450 mg/day, 7–12 months — 550 mg/day, 1–3 years — 800 mg/day, 3–7 years — 1100 mg/day day, 7–11 years – 1700 mg/day, 11–14 years – 1900 mg/day, 14–18 years – 2300 mg/day);
- iron (0–3 months — 4.0 mg/day, 7 months — 7 years — 10.0 mg/day, 7–11 years — 12.0 mg/day, 11–14 years — 12.0 mg/day for boys and 15.0 mg/day for girls, 14–18 years old - 15.0 mg/day for boys and 18.0 mg/day for girls);
- zinc (0-6 months - 3.0 mg/day, 7-12 months - 4.0 mg/day, 1-3 years - 5.0 mg/day, 3-7 years - 8.0 mg/day, 7–11 years – 10 mg/day, 11–18 years – 12.0 mg/day);
- iodine (0–12 months — 0.06 mg/day, 1–3 years — 0.07 mg/day, 3–7 years — 0.10 mg/day, 7–11 years — 0.12 mg/day, 11-14 years old - 0.13 mg/day for boys and 0.15 mg/day for girls, 14-18 years old - 0.15 mg/day);
- copper (0–6 months — 0.5 mg/day, 7–12 months — 0.3 mg/day, 1–3 years — 0.5 mg/day, 3–7 years — 0.6 mg/day, 7–11 years – 0.7 mg/day, 11–14 years – 0.8 mg/day, 14–18–1.0 mg/day);
- selenium (0–3 months — 0.01 mg/day, 4–12 months — 0.012 mg/day, 1–3 years — 0.015 mg/day, 3–7 years — 0.02 mg/day, 7–11 years - 0.03 mg/day, 11–14 years old — 0.04 mg/day, 14–18 years old — 0.05 mg/day);
- chromium (1-3 years - 11 mcg/day, 3-11 years - 15 mcg/day, 11-14 years - 25 mcg/day, 14-18 years - 35 mcg/day);
- fluoride (0–6 months — 1.0 mg/day, 7–12 months — 1.2 mg/day, 1–3 years — 1.4 mg/day, 3–7 years — 2.0 mg/day, 7-11 years old - 3.0 mg/day, 11-18 years old - 4.0 mg/day) [20].
The line of vitamin-mineral complexes for children includes Supradin Kids gel (from 3 years of age), Supradin Kids Junior (from 5 years of age), Supradin Kids gummy candies with omega-3 and choline (from 3 years of age), chewable lozenges Supradin Kids Bears (from 11 years of age).
Below we consider the composition of the complexes of the Supradin Kids line in relation to children of different ages (dosing and prescription in accordance with age indications - according to the manufacturer's instructions).
One teaspoon of Supradin Kids gel provides a 3-year-old child with 7.4 mcg of vitamin D (74% of the daily requirement), 1.9 mg of vitamin E (27.1%), 0.31 mg of vitamin B1 (34.4%) , 0.29 mg vitamin B2 (32.2%), 0.39 mg vitamin B6 (32.5%), 3.5 mg niacin (31.8%), 0.42 mg pantothenic acid (12%), 13.5 mg vitamin C (27%), plus 155 mcg ret. eq. β-carotene. It should be remembered that 6 mcg of the latter is considered equivalent to 1 mcg of vitamin A, that is, β-carotene in this case is essentially a substitute for retinol. Thus, for children over 3 years of age, 8 vitamins (2 fat-soluble and 6 water-soluble) are considered the most important. It should be noted that the inclusion of lecithin gel (100 mg in 1 teaspoon) in Supradin Kids gel not only optimizes the utilization of vitamin components of the complex, but also helps to increase concentration.
One chewable tablet of Supradin Kids Junior, offered to a 5-year-old child, contains 2.5 mcg of vitamin D3 (25% of the daily requirement), 300 mcg of vitamin A (60%), 5 mg of vitamin E (71.4%), 22 .5 mg ascorbic acid (45%), 6 mg nicotinamide (54.5%), 0.45 mg vitamin B1 (50%), 0.45 mg vitamin B2 (45%), 0.45 mg vitamin B6 (37 .5%), 0.5 mcg vitamin B12 (33.3%), 2 mg pantothenic acid (66.6%), 75 mcg folic acid (37.5%), 10 mcg biotin (66.6%), 120 mg calcium (13.3%), 25 mg magnesium (12.5%), 6 mg iron (60%), 4 mg zinc (50%), 0.4 mg copper (66.6%), 60 mcg iodine (60%), 12.5 mcg selenium (62.5%), 12.5 mcg chromium (83.3%). In addition, each tablet of Supradin Kids Junior contains 1 mg of manganese and 25 mg of choline (about 25% of the daily requirement for this vitamin-like substance). Mn deficiency, the norms of physiological consumption of which in childhood have not been established (for adults 2 mg/day), is accompanied by slower growth and increased fragility of bone tissue, which determines the advisability of subsidizing this microelement to children. It is noteworthy that this vitamin-mineral complex contains 12 vitamins out of 13 (with the exception of vitamin K), as well as 9 essential minerals. The described composition reflects modern ideas about the needs of children aged > 5 years for these micronutrients.
One gummy candy (lozenge) Supradin Kids with omega-3 and choline, taken by a 4-year-old child, provides him with 15 mg of vitamin C (30%), 4.5 mg of niacin (40.9%), 0.5 mg of vitamin B6 (41.6%) and 0.25 mcg vitamin B12 (8.3%). In addition, the composition contains docosahexaenoic omega-3 fatty acid (30 mg) and choline (30 mg); which helps improve memory and mental development of children [19]. The presence of Supradin Kids with omega-3 and choline of only the four water-soluble vitamins listed above is complemented by the addition of two biologically active substances, which actually turns this complex into a functional nutrition product.
Each chewable lozenge of Supradin Kids Bears taken by an 11-year-old child contains 2.5 mcg of vitamin D (25% of the daily requirement at this age), 400 mcg of vitamin A (40–50%%), 5 mg of vitamin E (41. 6%), 30 mcg vitamin C (42.8%), 1 mg vitamin B6 (58.8%), 0.5 mcg vitamin B12 (16.6%), 9 mg niacin (50%), 100 mcg folate acid (33.3%), 75 mcg biotin (300%). This (increased) presence of biotin is due to the important role of this vitamin in metabolism (participates in the synthesis of fats, gliogen, amino acid metabolism). The nine fat- and water-soluble vitamins listed above are among the most important for children moving from primary school to more complex and differentiated subject education. The vitamin composition of Supradin Kids Bears not only provides the child’s daily needs, but is also designed to stimulate mental development and learning ability [19].
There is no doubt about the need to recognize the importance of age differences in terms of children's needs for the most important micronutrients - vitamins, minerals, microelements. Not being sources of food energy, these micronutrients take part in the utilization of food (metabolism), regulation of the functions of various systems and organs, and implementation of the processes of growth, adaptation and development of the body [20].
Modern approaches to the development and composition of vitamin and vitamin-mineral complexes take into account the age characteristics of patients and are based on the awareness of the impossibility of providing children and adults with all the necessary vitamins and minerals exclusively through nutrition. Another feature of many multivitamin and vitamin-mineral complexes is the so-called “disease-specificity” and corrective focus, that is, therapeutic and preventive focus in relation to certain types of pathology (somatic or neuropsychiatric) [21, 22].
In fact, it should be recognized that the age-dependence and balance of vitamin-mineral complexes, as well as the inclusion in their composition of components with proven effectiveness (lecithin, choline, omega-3-unsaturated fatty acids, etc.), are fully consistent with the concept of neurodietology aimed at to optimize the treatment of psychoneurological diseases through qualitative/quantitative manipulation of the composition of diets, nutritional prevention of diseases of the nervous system, as well as to optimize psychomotor development, neurological and intellectual functions in children [22]. The role of vitamins and minerals in achieving this goal cannot be overestimated.
Literature
- Studenikin V.M., Shelkovsky V.I., Balkanskaya S.V. Possibilities of using vitamin-mineral complexes for preventive and therapeutic purposes in pediatric neurodietology / “Improving pediatric practice. From simple to complex": collection of articles. M., 2008. pp. 81–84.
- Studenikin V.M., Shelkovsky V.I. Vitamin and mineral complexes for children: a tool for neurodietology // Pediatrics. 2008. T. 87. No. 6. P. 105–109.
- Studenikin V. M. Hypovitaminosis and multivitamins // Issues of modern pediatrics. 2002. T. 1. No. 1. P. 48–51.
- Studenikin V.M. Hypovitaminosis // Attending Physician. 2002. No. 5. P. 52–55.
- Studenikin V.M., Kurbaytaeva E.M., Balkanskaya S.V., Vysotskaya L.M., Shelkovsky V.I. Vitamin and mineral complexes for children: the ABC of essential substances // Attending Physician. 2007. No. 2. pp. 91–93.
- Studenikin V.M., Balkanskaya S.V., Shelkovsky V.I., Kurbaytaeva E.M. Vitamin and mineral deficiency in children: somatic and psychoneurological aspects of the problem // Attending Physician. 2008. No. 1. P. 19–22.
- Studenikin V.M., Tursunkhuzhaeva S.Sh., Zvonkova N.G., Pak L.A., Shelkovsky V.I. Magnesium and its drugs in psychoneurology // Effective pharmacotherapy. Neurology and psychiatry. 2012. No. 4, p. 8–12, 58–60.
- Studenikin V.M., Tursunkhuzhaeva S.Sh., Kuzenkova L.M., Pak L.A., Shelkovsky V.I., Akoev Yu.S. Magnesium preparations in the correction of increased excitability in children // Farmateka. 2013. No. 7 (260). pp. 23–26.
- Studenikin V.M., Tursunkhuzhaeva S.Sh., Shelkovsky V.I. Zinc in neuropediatrics and neurodietology // Attending Physician. 2012. No. 1. pp. 44–47.
- Nikolaev A. S., Mazurina E. M., Kuznetsova G. V., Studenikin V. M., Chumakova O. V., Shelkovsky V. I., Maslova O. I. Physiological and pathophysiological significance of calcium metabolism in childhood // Question pract. pediatrics. 2006. T. 1. No. 2. P. 57–65.
- Studenikin V.M., Kurbaytaeva E.M. Calciopenic conditions and their correction // Attending Physician. 2010. No. 10. pp. 54–56.
- Studenikin V.M. Vitamin and vitamin-mineral complexes for pregnant women in Russia // Doctor.ru. 2005. No. 4. pp. 33–37.
- Studenikin V.M. Multivitamin preparations and vitamin-mineral complexes for pregnant women // Attending Doctor. 2007. No. 4. pp. 63–65.
- Studenikin V. M. Vitamin and mineral complexes for pregnant women: the basis for the formation of neurological health of mother and child // Attending Doctor. 2009. No. 3. P. 53–55.
- Studenikin V.M. Vitamins and multivitamin preparations in Russia // Doctor.ru. 2004. No. 3. P. 30–34.
- Studenikin V.M. Vitamins for children: myths and reality // Doctor.ru. 2004. No. 6. pp. 19–23.
- Studenikin V.M., Nikolaev A.S., Akoev Yu.S., Balkanskaya S.V., Gorelova Zh.Yu., Shelkovsky V.I. Vitamins and the use of multivitamin preparations in pediatrics // Pediatrician’s Handbook. 2006. No. 6. P. 68–88.
- Studenikin V.M., Balkanskaya S.V., Kurbaytaeva E.M., Vysotskaya L.M., Shelkovsky V.I. Multivitamin complexes for healthy and sick children // Pediatrician Practice. 2007. No. 5. pp. 12–14.
- Studenikin V. M. Possibilities of using multivitamin complexes in neuropediatrics // Treating Doctor. 2013. No. 9. pp. 60–64.
- Norms of physiological needs for energy and nutrients for various groups of the population of the Russian Federation. Method. rec. MP 2.3.1.2432–08.3.2.1. Balanced diet. M., 2008. 40 p.
- Studenikin V.M. Vitamin and mineral complex for the prevention of atherosclerosis and stroke // Attending Physician. 2014. No. 2. pp. 8–11.
- Neurodietology of childhood (collective monograph) / Edited by Studenikin V. M. M.: Dynasty. 2012, 672 p.
V. M. Studenikin, Doctor of Medical Sciences, Professor, Corresponding Member of the RAE
FSBI "NTsZD" RAMS, Moscow
Contact Information
What to eat?
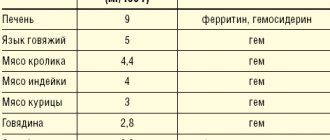
The main sources of phosphorus are animal products: meat and milk. If a person strives to maintain an optimal balance of calcium in the body, phosphorus is usually enough for him. The highest levels of phosphorus are found in chicken, beef, fish, dairy products and eggs. For every gram of animal protein there is 12 to 15 mg of phosphorus. There is a lot of phosphorus in nuts, cereals and beans, but it is absorbed worse from plant foods than from animal foods, since it is mainly contained in the chemical compound phytin, which the human body does not absorb. Keep this in mind if you decide to give up animal products. Fruits and vegetables contain very little phosphorus.
Why is phosphorus deficiency dangerous?
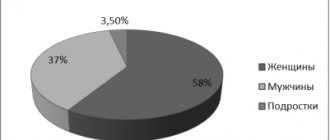
The body can experience a deficiency of this microelement for various reasons. But most often he declares himself in such situations:
- During fasting. Especially when a person goes on a diet that involves mainly consuming plant foods.
- For food poisoning.
- Metabolic disorders caused by dysfunction of the kidneys, thyroid gland, excessive consumption of alcohol, carbonated drinks, and excess blood sugar.
- In pregnant women, as well as during lactation.
- In people who systematically experience heavy physical activity.
- With insufficient consumption of phosphorus-containing products.
- With an excess of barium, aluminum, magnesium and calcium, which together with phosphorus form insoluble compounds. In this combination, phosphorus loses its ability to actively participate in metabolic processes.
- The presence of chronic renal pathologies.
The deficiency of this microelement can be determined by the corresponding symptoms:
- weakened immune system, susceptibility to colds;
- development of rickets and periodontal disease;
- skin diseases;
- loss of appetite, exhaustion;
- mental disorders, anxiety;
- general weakness, loss of concentration;
- severe pain in muscles, bones, joints;
- memory impairment, depression;
- weight loss or gain.
Of course, similar symptoms can accompany a number of common diseases. Therefore, to make sure that your problem is a lack of phosphorus, you should consult your doctor. After all, if the body experiences a significant deficiency of this element for a long time, negative manifestations become a natural result. Therefore, it is necessary to know which foods contain a lot of phosphorus and compensate for its deficiency with the help of a well-designed daily diet.
Patient preparation rules
urine
Notes:
Any portion of urine, regardless of the time of day, is collected after toileting the external genitalia.
daily urine Notes:
Perform the first morning urination in the toilet. Collect all further daily urine, including the morning portion of the next day, into a container (important - the volume of the container must be sufficient for the expected amount of urine per day). During the entire collection period, keep biological material in a cool place, protected from light. After the collection is completed, determine the daily volume of collected urine, mix, pour 30-40 ml into a standard urine container and deliver to the ML DILA department within 2 hours after collecting the last portion.
You can add this study to your cart on this page
References
- Simerville, J., Maxted, W., Pahira, J. Urinalysis: a comprehensive review. Am Fam Physician., 2005. - Vol. 71(6). - P. 1153-62.
- Chernecky, C., Berger, B. et al. Laboratory Tests and Diagnostic Procedures. Saunder Elsevier, 2008.
- Fauci, A., Ksper, D., Longo, E. et al. Harrison's principles of internal medicine. The McGraw-Hill Companies, 2008.
- Pettifor, J. What's new in hypophosphataemic rickets? Eur J Pediatr., 2008. - Vol. 167(5). - P. 493-9.
- Wolf, M. Forging forward with 10 burning questions on FGF23 in kidney disease. J AmSocNephrol., 2010. - Vol. 21(9). - P. 1427-35.
Interpretation:
- Hyperparathyroidism; vitamin D-resistant rickets; immobilization after paraplegia or fracture; vitamin D intoxication; damage to the renal tubules (for example, Fanconi syndrome); familial hypophosphatemia; non-renal acidosis (increased excretion of phosphates as a buffer for urine); predisposition to the formation of urinary stones; leukemia
- Hypoparathyroidism; pseudohypoparathyroidism; parathyroidectomy; acromegaly; bone metastases; infectious diseases, in particular tuberculosis; acute yellow atrophy.
Sample result (PDF)
Interference:
- Anabolic steroids, androgens, beta-blockers (eg, acebutol, pindolol), estrogens, ergocalciferol, furosemide, growth hormone, hydrochlorothiazide, methicillin (for nephrotoxicity), phosphates, sodium etidronate, tetracycline (for nephrotoxicity),
- Acetazolamide, albuterol, aluminum-containing antacids, amino acids, anesthetics, calcitonin, carbamazepine, epinephrine, estramustine, fructose, glucocorticoids, glucose, hydrochlorothiazide (long-term use), ifosfamide, insulin, isoniazid, oral contraceptives, phenytoin, sucralfate