If, as a result of a pathological process, deformation of the valve tissue occurs and the hole through which blood enters the next part of the heart narrows, then such a defect is called stenosis. Deformation can lead to the heart valves not closing due to changes in shape, shortening them as a result of scarring of the affected tissues; this defect is called insufficiency. Valve insufficiency can be functional, resulting from stretching of the chambers of the heart; the area of the unchanged valve is not enough to close the enlarged hole - the leaflets sag (prolapse).
The work of the heart is restructured depending on the changes that have occurred and the needs of blood flow in the body.
Causes of acquired heart defects
In most cases, the defects are caused by rheumatic diseases, in particular rheumatic endocarditis (about 75% of cases). The cause may also be the development of atherosclerosis, systemic connective tissue diseases, trauma, sepsis, infections, overload, and autoimmune reactions. These pathological conditions cause disturbances in the structure of the heart valves.
Classification of acquired heart defects
The human heart has four chambers: the left and right atria and ventricles, between which are the heart valves. The aorta emerges from the left ventricle, and the pulmonary artery emerges from the right ventricle.
Between the left heart chambers is a bicuspid valve, the mitral valve. And between the right sections there is a tricuspid valve, another name is tricuspid. In front of the aorta there is the aortic valve, in front of the pulmonary artery there is another valve, the pulmonary valve.
The performance of the heart muscle depends on the functioning of the valves, which, when the heart muscle contracts, allow blood to flow into the next section without obstruction, and when the heart muscle relaxes, do not allow blood to flow back. If the function of the valves is impaired, the function of the heart is also impaired.
Based on the reasons for their formation, defects are classified as follows:
- degenerative, or atherosclerotic, they occur in 5.7% of cases; More often, these processes develop after forty to fifty years, calcium is deposited on the leaflets of the damaged valves, which leads to the progression of the defect;
- rheumatic, formed against the background of rheumatic diseases (in 80% of cases);
- defects that arise as a result of inflammation of the inner lining of the heart (endocarditis);
- syphilitic (in 5% of cases).
Based on the type of functional pathology, defects are divided into the following types:
- simple – valve insufficiency or stenosis;
- combined – insufficiency or narrowing of two or more valves;
- combined - both pathologies on one valve (stenosis and insufficiency).
Depending on the location, the following pathologies are distinguished:
- mitral valve disease;
- tricuspid defect;
- aortic defect.
Hemodynamics can be impaired to varying degrees:
- insignificant;
- moderately;
- expressed.
The mitral valve is affected more often than the aortic valve. Pathologies of the tricuspid valve and pulmonary valve are less common.
Degrees of regurgitation
Another basis for classification is the degree of deviation from the norm. Also called stages of the pathological process.
Accordingly, they distinguish:
- Weakly expressed type. 1st degree. The amount of blood returning is not known exactly. The volumes of the jet do not exceed 1 cm in diameter. The intensity of manifestations with minimal tricuspid regurgitation is insignificant or completely absent, which makes early diagnosis a matter of luck. This is the best time to start therapy under the supervision of cardiac surgeons.
- Moderate type. 2nd degree. Characterized by disruption of normal blood flow in a volume of 2 cm, no more. Recovery is carried out surgically. The clinical picture is minimal, characterized by chest pain, shortness of breath during intense physical activity. There is a chance for a complete cure, the likelihood of the formation of persistent cardiac and extracardiac defects is present, but it is not yet great. Even if these occur, the likelihood of a high-quality, long life is maximum.
- Expressed type. 3rd degree. A stream of blood more than 2 cm in diameter. Chronic heart failure of congestive type develops. There are prospects for recovery, but they are not complete, and long-term, lifelong maintenance therapy is required.
- Terminal phase. 4th degree. Surgical assistance does not make much sense, since the heart, kidneys, liver, and brain are significantly changed. Recovery is impossible; palliative care is required to ensure an acceptable quality of life for the short remaining period of life. Death occurs from acute heart failure.
Classifications are used to accurately assess the patient’s condition, prospects for treatment, and determine diagnostic and therapeutic tactics.
Symptoms of acquired heart defects
Mitral stenosis
It manifests itself as compaction or fusion of the leaflets, a decrease in the area of the mitral valve opening. As a result, the flow of blood from the left atrium to the left ventricle is obstructed, and the left atrium begins to work with increased load. This leads to enlargement of the left atrium. The left ventricle receives less blood.
Due to the decrease in the area of the mitral orifice, the pressure in the left atrium increases, and then in the pulmonary veins, through which oxygenated blood flows from the lungs to the heart. Typically, the pressure in the pulmonary arteries begins to increase when the diameter of the opening becomes less than 1 cm, compared to the normal 4-6 cm, and a spasm occurs in the arterioles of the lungs, which aggravates the process. Thus, so-called pulmonary hypertension is formed, the long-term existence of which leads to sclerosis of arterioles with their obliteration, which cannot be eliminated even after eliminating the stenosis.
With this defect, first of all, the left atrium hypertrophies and expands, and then the right parts of the heart.
At the beginning of the formation of this defect, the symptoms are little noticeable. Subsequently, shortness of breath, cough during physical activity, and then at rest come first. Hemoptysis, persistent pain in the heart, and rhythm disturbances (tachycardia, atrial fibrillation) may occur. If the process goes far, then pulmonary edema may develop during physical activity.
There are physical signs of mitral stenosis: diastolic murmur in the heart, a trembling of the chest corresponding to this noise is felt (“cat purring”), and the boundaries of the heart change. An experienced specialist can often make a diagnosis after a careful examination of the patient.
Mitral regurgitation
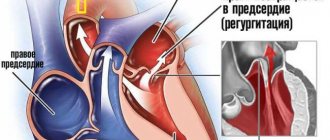
Valve insufficiency is expressed in the ability of blood to return back into the atrium during contraction of the left ventricle, since a message remains between the left atrium and the ventricle, which is not closed by the valve leaflets at the time of contraction. Such insufficiency is caused either by deformation of the valve as a result of a tissue-changing process, or by its sagging (prolapse), due to stretching of the chambers of the heart when they are overloaded.
Compensated mitral regurgitation usually lasts for several years; in the affected heart, the work of the left atrium and left ventricle increases, first hypertrophy of the muscles of these parts develops, and then the cavities begin to expand (dilatation). Then, due to a decrease in stroke volume, the minute ejection of blood from the heart begins to decrease, and the amount of blood returning (regurgitation) to the left atrium increases. Blood stagnation begins in the pulmonary circulation (pulmonary), the pressure in it increases, the load on the right ventricle increases, it hypertrophies and expands. This leads to rapid decompensation of cardiac activity and the development of right ventricular failure.
If compensatory mechanisms do not have time to develop in acute mitral valve insufficiency, the disease can begin with pulmonary edema and lead to death.
Clinical manifestations of mitral regurgitation in the compensated stage are minimal and may not be noticed by the patient. Beginning decompensation is characterized by shortness of breath, poor tolerance to physical activity, then, when stagnation in the pulmonary circulation increases, attacks of cardiac asthma appear. In addition, pain in the heart area, palpitations, and interruptions in heart function may bother you.
Right ventricular heart failure leads to stagnation of blood in the systemic circulation. The liver becomes enlarged, cyanosis of the lips and limbs appears, swelling in the legs, fluid in the abdomen, heart rhythm disturbances (50% of patients have atrial fibrillation).
It is not difficult to make a diagnosis of mitral regurgitation at present with the available instrumental research methods: ECG, ECHO-CG, radiation diagnostic methods, ventriculography and others. However, an examination by an attentive cardiologist based on anamnesis, auscultation, percussion, and palpation will allow you to draw up the correct examination algorithm and timely take measures to prevent further development of the process of formation of the defect.
Aortic stenosis
This defect among PPS is detected quite often, in 80-85% of cases it is formed as a result of rheumatism, in 10-15% of cases it is acquired against the background of an atherosclerotic process, with subsequent deposition of calcium in atherosclerotic plaques (calcinosis). There is a narrowing of the aortic orifice at the site of the semilunar valve of the aorta. For many years, the left ventricle works with increasing tension, however, when the reserves are depleted, the left atrium, the pulmonary circle, and then the right parts of the heart begin to suffer. The pressure gradient between the left ventricle and the aorta increases, which is directly related to the degree of narrowing of the opening. The ejection of blood from the left ventricle becomes less, the blood supply to the heart deteriorates, which is manifested by angina pectoris, low blood pressure and weak pulse, cerebrovascular insufficiency with neurological symptoms, including dizziness, headache, loss of consciousness.
The appearance of complaints in patients begins when the area of the aortic mouth decreases by more than half. When complaints appear, this indicates an advanced process, a high degree of stenosis and a high pressure gradient between the left ventricle and the aorta. In this case, treatment should be discussed taking into account surgical correction of the defect.
Aortic insufficiency
- this is a valve pathology in which the outlet from the aorta is not completely blocked; blood has the ability to flow back into the left ventricle during its relaxation phase. The walls of the ventricle thicken (hypertrophy) as more blood has to be pumped. With ventricular hypertrophy, insufficiency of its nutrition gradually manifests itself. More muscle mass requires more blood flow and oxygen supply. At the same time, due to the fact that part of the blood in diastole returns to the left ventricle, the aortic-left ventricular gradient decreases (it is what determines the coronary blood flow) and, as a result, less blood enters the arteries of the heart. Angina occurs. There are sensations of pulsation in the head and neck. Neurological manifestations are characteristic, such as: lightheadedness, dizziness, sudden fainting, especially during physical exertion, when changing body position. The hemodynamics of the systemic circulation with this defect are characterized by: high systolic pressure, low diastolic pressure, compensatory tachycardia, increased pulsation of the croup
ny arteries, including the aorta. During the decompensation stage, dilatation (expansion) of the left ventricle develops, the efficiency of systole decreases, the pressure in it increases, then in the left atrium and pulmonary circulation. Clinical signs of stagnation in the pulmonary circulation appear: shortness of breath, cardiac asthma.
A thorough examination by a cardiologist may allow the doctor to suspect or even diagnose aortic insufficiency. Well-known symptoms such as “carotid dance” - increased pulsation of the carotid arteries, “capillary pulse”, which is detected by pressing on the nail phalanx, de Musset’s symptom - when the patient’s head sways in time with the phases of the cardiac cycle, pulsation of the pupils and others are detected already at the stage a far advanced process. But palpation, percussion, auscultation and careful history taking will help identify the disease at earlier stages and prevent the progression of the disease.
Tricuspid stenosis
This defect rarely occurs as an isolated pathology. It is expressed in the narrowing of the existing opening between the right ventricle and the right atrium, which are separated by the tricuspid valve. Most often it occurs with rheumatism, infective endocarditis and other systemic connective tissue diseases; sometimes there is a narrowing of the opening as a result of the formation of a myxoma-tumor formed in the right atrium, less often there are other reasons. Gamodynamics are disrupted as a result of the fact that not all the blood from the atrium can enter the right ventricle, which normally should occur after atrial systole. The atrium becomes overloaded, stretched, blood stagnates in the systemic circulation, the liver enlarges, swelling of the lower extremities and fluid appear in the abdominal cavity. Less blood flows from the right ventricle to the lungs, which causes shortness of breath. In the initial stage, there may be no symptoms; these hemodynamic disorders arise later - heart failure, atrial fibrillation, thrombosis, cyanosis of the nails, lips, yellowness of the skin.
Tricuspid insufficiency. This pathology most often accompanies other defects and manifests itself in the form of tricuspid valve insufficiency. Due to venous stagnation, ascites gradually develops, the liver and spleen increase in size, high venous pressure is noted, liver fibrosis develops and a decrease in its function.
Forms of violation
Typification of the pathological process is carried out on two grounds.
Based on the origin of the anatomical defect, they talk about:
- Primary form. It develops spontaneously, against the background of cardiac problems themselves. Including aortic insufficiency, previous inflammatory, infectious conditions and others.
It is characterized by greater complexity from the point of view of cure and prospects for recovery, since correction requires not only the symptomatic component, but also the acquired defect.
This group also includes congenital factors caused by genetic defects and spontaneous deformations of the tricuspid valve.
- Secondary variety. Against the background of current pathologies of distant organs and systems.
Methods for diagnosing heart defects
In order to establish a diagnosis of heart disease, an anamnesis is collected, the presence of diseases that could lead to deformation of the heart valve is revealed: rheumatic diseases, infectious, inflammatory processes, autoimmune diseases, injuries.
- The patient must be examined to identify the presence of shortness of breath, cyanosis, edema, and pulsation of peripheral veins. Using percussion, the boundaries of the heart are identified and sounds and murmurs in the heart are listened to. The size of the liver and spleen is determined.
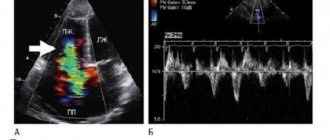
- The main method for diagnosing valve pathology is echocardiography
, which allows you to identify the defect, determine the area of the opening between the atrium and the ventricle, the size of the valves, cardiac fraction, pressure in the pulmonary artery.
More accurate information about the condition of the valves can be obtained by performing transesophageal echocardiography. - Electrocardiography is also used in diagnostics, which allows one to assess the presence of atrial and ventricular hypertrophy and identify signs of overload of the heart. Daily Holter ECG monitoring allows you to identify rhythm and conduction disturbances.
- Highly informative methods for diagnosing heart defects are cardiac MRI or cardiac MSCT. Computed tomography scans provide precise and numerous sections, which can be used to accurately diagnose the defect and its type.
- Laboratory tests play an important role in diagnosis, including urine and blood tests, determination of blood sugar, cholesterol levels, and rheumatoid tests. Laboratory tests allow us to identify the cause of the disease, which plays an important role in subsequent treatment and patient behavior.
How to get treatment in Israel
By choosing our multidisciplinary complex, you get the opportunity to visit the right specialists and undergo all types of diagnostics in one place. Our own developments and exchange of experience with foreign partners make our clinic one of the best in the world.
To avoid the costs of intermediaries, use our official website. You can submit a request to visit the children's cardio center by filling out an electronic form. A Russian-speaking representative of the international department will contact you within two hours and answer all questions.
Prevention and prognosis for PPS
There are no preventive measures that would protect one hundred percent from acquired heart disease. But there are a number of measures that will reduce the risk of developing heart defects. This means the following:
- timely treatment of infections caused by streptococcus (in particular tonsillitis);
- bicillin prophylaxis in the event of a rheumatic attack;
- taking antibiotics before surgical and dental procedures if there is a risk of infective endocarditis;
- prevention of syphilis, sepsis, rheumatism: sanitation of infectious foci, proper nutrition, work and rest schedule;
- rejection of bad habits;
- presence of moderate physical activity, accessible physical exercises;
- hardening.
The prognosis for the life and ability to work of people with heart defects depends on the general condition, fitness of the person, and physical endurance. If there are no symptoms of decompensation, a person can live and work as usual. If circulatory failure develops, work should either be lightened or stopped; sanatorium treatment at specialized resorts is indicated.
It is necessary to be observed by a cardiologist in order to monitor the dynamics of the process and, as the disease progresses, to promptly determine the indications for cardiac surgical treatment of heart disease.
How much does it cost to treat tricuspid valve insufficiency in children in Israel?
Hadassah is considered one of the best medical institutions in Israel. The most effective methods for recognizing and combating children's heart defects are being developed and implemented here; qualified senior and mid-level physicians work here.
The administration of the medical complex has a competitive pricing policy, so our cost of stay is average across the country and is 20–30% lower than in Europe and America. In addition, all prices are controlled by the Israeli Ministry of Health.
Treatment of acquired heart defects can be conservative or surgical
Conservative treatment is effective only in the early stages of the development of heart disease and requires mandatory follow-up by a cardiologist.
PPS should be treated surgically when:
- Heart failure progresses.
- Pathological changes in the valve significantly affect hemodynamics.
- The ongoing conservative therapy does not have the desired effect.
- And there are fears of serious complications.
Types of operations for heart defects
Open heart surgery is performed under artificial circulation through a median sternotomy. Median sternotomy creates optimal conditions for the cardiac surgeon to perform the necessary surgical interventions for various pathologies and to connect the heart-lung machine. The soft tissue incision is approximately equal in length to the length of the sternum (about 20 cm), and the sternum is dissected along its entire length.
The main two types of operations that are currently used for PPS are reconstruction of the affected valves (plastic) or their prosthetics.
Valve-sparing surgery
Performed to eliminate the cause of valve dysfunction.
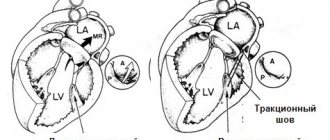
If the valves do not close (valve insufficiency), then the cardiac surgeon during the operation achieves normalization of the closure of the valve leaflets, performing resection of the valve leaflets, annuloplasty, commissural plastic surgery, and chord replacement. If there is valve stenosis, then the sections of the valves that have fused due to a pathological process are separated and an open commissurotomy is performed.
Valve replacement surgery
If it is impossible to perform plastic surgery, when there are no conditions for this, valve replacement operations for prosthetic heart valves are performed. In case of intervention on the mitral valve, replacement is performed with full or partial preservation of the anterior or posterior valve leaflets, and if impossible, without their preservation.
In valve replacement surgeries, prostheses are used.
- Prosthetics can be made from animal or human tissue. Such prostheses are called biological. Its main advantage is that the patient does not need to take anticoagulant drugs during subsequent years of life, and their main disadvantage is their limited service life (10-15 years).
- Prostheses consisting entirely of mechanical elements (titanium and pyrolytic carbon) are called mechanical. They are very reliable and can serve without failure for many years, without replacement, but after such an operation the patient must always take anticoagulants for life, this is a negative aspect of using a mechanical prosthesis.
Minimally invasive surgeries
Modern surgery, thanks to the creation of new instruments, has the opportunity to modify surgical approaches to the heart, which leads to operations becoming minimally traumatic for the patient.
The point of such operations is that access to the heart is carried out through small incisions in the skin. During minimally invasive operations on the mitral valve, a right-sided lateral minithoracotomy is performed, with a skin incision of no more than 5 cm, this allows one to completely avoid dissecting the sternum and provides convenient access to the heart. To improve visualization, endoscopic video support with multiple magnification is used. With minimally invasive access to the aortic valve, the skin incision is approximately half as large (incision length 8 cm), and the sternum is incised lengthwise in its upper part. The advantage of this method is that the uncut portion of the sternum provides greater stability after surgery, as well as a better cosmetic effect by reducing the size of the suture.
Endovascular operations - transcatheter aortic valve replacement (TAVI).
Methods of transcatheter aortic valve implantation:
- The entire operation is carried out through a blood vessel (femoral or subclavian artery). The meaning of the procedure is to puncture the femoral or subclavian artery with a guide catheter and deliver the stent valve against the blood flow to the site of its implantation (aortic root).
- Through the aorta. The essence of the method is to dissect the sternum over a short distance (ministernotomy) and puncture the aortic wall in the ascending section and implantation of a stent valve into the aortic root. The method is used when it is impossible to deliver the valve through the femoral and subclavian arteries, as well as when there is a pronounced bend in the arterial arch.
- Through the apex of the heart. The meaning of the procedure is to make a small incision in the fifth intercostal space on the left (minithoracotomy), puncture the apex of the heart with a guide catheter and install a stent valve. Once the new valve is implanted, the catheter is removed. The new valve starts working immediately.
There are two types of stent valves:
- Self-expanding stent-valve expands to the desired size after removing the restrictive sleeve sleeve from it.
- A balloon-dilatable stent valve that expands to the desired size when the balloon is inflated; After final installation of the stent valve, the balloon is deflated and removed.
To determine whether TAVI surgery is appropriate, the patient must undergo a series of tests, including an ECG, echocardiography, computed tomography (CT) scan, and angiography.
Currently, the TAVI procedure is increasingly used not only for aortic stenosis, but also for aortic insufficiency, as well as their combination. In addition, TAVI surgery is used for dysfunction of the biological prosthetic aortic valve.
TAVI surgery is performed under general anesthesia and requires a multidisciplinary approach. The procedure is performed by a specialized team, which includes an interventional cardiologist, cardiac surgeon, anesthesiologist, and radiologist.
The presence of a stent valve is not an indication for the patient to take the indirect anticoagulant Warfarin (in the absence of other indications).
Rehabilitation after treatment of tricuspid valve insufficiency in children
The recovery period takes place in the specialized rehabilitation department of the Hadassah MC. They use a modern approach and innovative technologies that promote a speedy recovery and return to a full life.
To prevent negative consequences upon discharge, Israeli cardiologists recommend following certain requirements:
- follow all doctor's instructions;
- refuse self-medication;
- exclude independent withdrawal of medications or changes in their dosage;
- After complete recovery, start hardening the child.
The equipment of the rehabilitation center allows both children and their accompanying persons to stay comfortably in our institution.
Forecast
{banner_banstat9}
Depends on the stage and nature of therapy.
- At the first stage, the survival rate is 100%, especially if there is no progression of the condition.
- The second is associated with a probability of 85%.
- Third - 45%.
- The fourth or terminal puts an end to the patient, giving no chance. The median is 1-2 years, often even less.
When carrying out complex therapy, it is possible to stabilize the conditions of even the most severe patients, prolonging life for several years.
Favorable prognostic factors:
- Period of youth.
- Absence of somatic pathologies, bad habits, complications after the operation.
- Good family history.
- Response to treatment.
- Reduction of symptoms.
Determining the possible outcome falls on the shoulders of the cardiologist. In order to say anything concrete, you need to at least carry out a full diagnosis.
Preparation for valve repair
The first step in patient preparation is diagnosis. To clarify the diagnosis, a chest ultrasound, ECG, blood and urine tests are prescribed. In some modern clinics, the heart is examined using a computed tomograph. Angiography of the heart vessels and or CT scans show the heart muscle and blood circulation in detail; during the studies, the radiologist can accurately determine tricuspid stenosis or insufficiency. After the tests, the patient undergoes a consultation with a cardiac surgeon, neurologist, and therapist.
If valve disorders are accompanied by additional heart problems, they try to get rid of them before surgery. For example, in case of arrhythmia, the heart rhythm is first normalized. If the clinical picture is complicated by heart failure, a sodium-excluding diet is prescribed. All patients are prescribed a diet a few days before the procedure; they need to avoid salt, too fatty foods, too spicy foods, and drink less water. You cannot eat 8 hours before plastic surgery. As part of the patient's preparation, the attending doctor explains to his patient how tricuspid valve repair is performed. It is important that the person being operated on does not worry and does not overload the heart and nervous system. If you have concerns or fears, you should talk to your doctor about it.
Plastic results
Symptoms of stenosis or tricuspid insufficiency disappear immediately after surgery. In the first 1-2 months after it, the patient’s condition will gradually improve if the manipulations went without complications. Negative consequences may include:
- bleeding;
- heart attack;
- formation of blood clots and blockage of blood vessels;
- disturbances of vision, appetite, sleep (this is normal, goes away within a month);
- infection;
- hemolytic anemia.
Best materials of the month
- Coronaviruses: SARS-CoV-2 (COVID-19)
- Antibiotics for the prevention and treatment of COVID-19: how effective are they?
- The most common "office" diseases
- Does vodka kill coronavirus?
- How to stay alive on our roads?
To prevent such consequences, scheduled and unscheduled inspections are prescribed. In most cases, the prognosis for tricuspid valve surgery is positive, heart function is restored, and the patient returns to his normal lifestyle.
The postoperative period is complicated by the use of anticoagulants, which reduce blood clotting. Biological implants do not require constant use of anticoagulants, but the lifespan of such prostheses is limited. Observations of patients show that a biological implant lasts an average of 9-10 years.
Mechanical analogues have a long service life; they keep the heart functioning for 20-25 years. But during this entire time you need to take medications that reduce blood clotting. When the life of the implant has passed, it is replaced with the next one. If regular sutures were used during plastic surgery, reoperation may not be necessary. However, long-term patient survival is higher with rings than with conventional suture techniques.
How dangerous is the disease?
Complications arise starting from the third, less often the second stage of the pathological process. Tricuspid valve regurgitation determines the following consequences for health and life:
- Acute heart failure. Disruption of the normal functioning of cardiac structures. It is characterized by a triad of signs: a decrease in blood output, a drop in local and generalized hemodynamics, and arrhythmic processes. It has a short period of development in an acute case; in a latent course, the duration of formation of a full-fledged picture is 2-4 weeks; death occurs as a result of stopping the work of a muscular organ.
- Cardiogenic shock. The condition is lethal in almost 100% of cases. There is no prospect of cure. Even with partial recovery, there is a guarantee of a repeat episode.
- Heart attack. Myocardial nutritional disturbances, acute tissue necrosis and, as a result, decreased functional activity. Heart failure develops with all its consequences.
- Stroke. Cerebral ischemia.
- Dangerous forms of arrhythmia leading to cardiac arrest.
Minor regurgitation provokes fatal complications in 0.3-2% of cases, often the result of a random coincidence.
Hemodynamically significant forms determine the risk of death in a wide range: from 10 to 70% and higher.
The main cause of death is not regurgitation, but organic defects of the heart and systems developing against its background.