Pharmacological properties of the drug Lozap
Losartan is a specific antagonist of the receptor (AT1 type) of angiotensin II. Angiotensin II binds to the AT1 receptor, which is found in many tissues (eg vascular smooth muscle, adrenal glands, kidneys and heart). Losartan and its pharmacologically active metabolite carboxylic acid (E-3174) block the effects of angiotensin II. Losartan does not bind or block other hormone receptors and ion channels important for cardiovascular regulation. Losartan does not inhibit ACE, but blocks the response to angiotensin I and II and has no effect on the kinin system or bradykinin levels. Losartan has no effect on autonomic reflexes and the level of norepinephrine in the blood plasma. The drug is equally effective in men, women under 65 years of age and in elderly and senile patients with hypertension (arterial hypertension). With simultaneous use of Lozap with thiazide-type diuretics, the degree of blood pressure reduction increases. After oral administration, losartan is well absorbed and, as a result of metabolism during the initial passage through the liver, an active metabolite of carboxylic acid and inactive metabolites are formed. Systemic bioavailability after oral administration of losartan is about 33%. The average maximum concentration of losartan is achieved within 1 hour, and its active metabolite - within 3-4 hours. When using the drug with a standardized diet, no clinically significant effect on the profile of the concentration of losartan in the blood plasma was noted. Plasma clearance for losartan and its active metabolite is approximately 600 and 50 ml/min, respectively. The renal clearance of losartan and its active metabolite is about 74 and 26 ml/min, respectively. After oral administration, almost 4% of the dose is excreted unchanged in the urine and about 6% of the dose as an active metabolite. With oral administration of losartan potassium in doses up to 200 mg, the pharmacokinetics of the drug and its active metabolite are linear. After oral administration, the concentration of the drug and its active metabolite in the blood plasma decreases polyexponentially with a final half-life of 2 hours for losartan and 6–9 hours for the active metabolite. At a single daily dose of 100 mg, neither losartan nor its active metabolite accumulates in the blood plasma in significant quantities.
Lozap® Plus
Hydrochlorothiazide
Renal dysfunction
In patients with impaired renal function, hydrochlorothiazide may cause azotemia. In case of renal failure, accumulation of hydrochlorothiazide is possible.
In patients with reduced renal function, periodic monitoring of creatinine clearance is necessary. If renal dysfunction progresses and/or oliguria (anuria) occurs, hydrochlorothiazide should be discontinued.
Liver dysfunction
When using thiazide diuretics in patients with impaired liver function, hepatic encephalopathy may develop. In patients with severe liver failure or hepatic encephalopathy, the use of thiazides is contraindicated. In patients with mild to moderate hepatic impairment and/or progressive liver disease, hydrochlorothiazide should be used with caution, since even slight changes in fluid electrolyte balance and ammonium accumulation in the blood serum can cause hepatic coma. If symptoms of encephalopathy occur, diuretics should be discontinued immediately.
Water-electrolyte balance and metabolic disorders
Thiazide diuretics (including hydrochlorothiazide) can cause a decrease in the volume of circulating fluid (hypovolemia) and disturbances in water and electrolyte balance (including hypokalemia, hyponatremia, hypochloremic alkalosis). Clinical symptoms of fluid and electrolyte imbalance include dry mouth, thirst, weakness, lethargy, fatigue, drowsiness, restlessness, muscle pain or cramps, muscle weakness, marked decrease in blood pressure, oliguria, tachycardia, arrhythmia and gastrointestinal disorders (such as nausea and vomiting). In patients receiving hydrochlorothiazide therapy (especially with long-term course treatment), clinical symptoms of water-electrolyte imbalance should be identified and blood electrolyte levels should be regularly monitored.
Sodium
All diuretics can cause hyponatremia, sometimes leading to severe complications. Hyponatremia and hypovolemia can lead to dehydration and orthostatic hypotension. A concomitant decrease in chlorine ions can lead to secondary compensatory metabolic alkalosis, but the frequency and severity of this effect are insignificant. It is recommended to determine the content of sodium ions in the blood plasma before starting treatment and regularly monitor this indicator while taking hydrochlorothiazide.
Potassium
When using thiazide and thiazide-like diuretics, there is a risk of a sharp decrease in the potassium content in the blood plasma and the development of hypokalemia (potassium concentration less than 3.4 mmol/l). Hypokalemia increases the risk of developing heart rhythm disturbances (including severe arrhythmias) and enhances the toxic effect of cardiac glycosides. In addition, hypokalemia (as well as bradycardia) is a condition that contributes to the development of polymorphic ventricular tachycardia of the “pirouette” type, which can be fatal.
Hypokalemia poses the greatest danger to the following groups of patients: elderly people, patients simultaneously receiving therapy with antiarrhythmic and non-antiarrhythmic drugs that can cause polymorphic ventricular tachycardia of the "pirouette" type or increase the duration of the QT interval on the ECG, patients with impaired liver function, coronary heart disease , chronic heart failure. In addition, patients with an increased QT interval are at increased risk. It does not matter whether this increase is caused by congenital causes or the effect of drugs.
In all the cases described above, it is necessary to avoid the risk of developing hypokalemia and regularly monitor the potassium content in the blood plasma. The first measurement of the content of potassium ions in the blood must be carried out within the first week from the start of treatment. If hypokalemia occurs, appropriate treatment should be prescribed. Hypokalemia can be corrected by using potassium-containing medications or eating foods rich in potassium (dried fruits, fruits, vegetables).
Calcium
Thiazide diuretics may reduce the excretion of calcium ions by the kidneys, leading to a slight and temporary increase in plasma calcium levels. In some patients, with long-term use of thiazide diuretics, pathological changes in the parathyroid glands were observed with hypercalcemia and hyperphosphatemia, but without the typical complications of hyperparathyroidism (nephrolithiasis, decreased bone mineral density, peptic ulcer). Severe hypercalcemia may be a manifestation of previously undiagnosed hyperparathyroidism.
Because of their effect on calcium metabolism, thiazides may interfere with laboratory parameters of parathyroid function. Thiazide diuretics (including hydrochlorothiazide) should be discontinued before testing parathyroid function.
Magnesium
Thiazides have been found to increase renal excretion of magnesium, which can lead to hypomagnesemia. The clinical significance of hypomagnesemia remains unclear.
Glucose
Treatment with thiazide diuretics may impair glucose tolerance. When using hydrochlorothiazide in patients with manifest or latent diabetes mellitus, it is necessary to regularly monitor the concentration of glucose in the blood. Dosage adjustment of hypoglycemic medications may be required.
Uric acid
In patients with gout, the frequency of attacks may increase or the course of gout may worsen. Careful monitoring of patients with gout and impaired uric acid metabolism (hyperuricemia) is necessary.
Lipids
When using hydrochlorothiazide, the concentration of cholesterol and triglycerides in the blood plasma may increase.
Acute myopia/secondary angle-closure glaucoma
Hydrochlorothiazide can cause an idiosyncratic reaction, leading to the development of acute myopia and an acute attack of secondary angle-closure glaucoma. Symptoms include: sudden loss of visual acuity or eye pain, usually occurring within hours to weeks of starting hydrochlorothiazide therapy. If left untreated, acute angle-closure glaucoma can lead to irreversible vision loss. If symptoms appear, you should stop taking hydrochlorothiazide as soon as possible. If intraocular pressure remains uncontrolled, emergency medical treatment or surgery may be required. Risk factors for the development of acute angle-closure glaucoma are: a history of an allergic reaction to sulfonamides or penicillin.
Immune system disorders
There are reports that thiazide diuretics (including hydrochlorothiazide) can cause exacerbation or progression of systemic lupus erythematosus, as well as lupus-like reactions.
In patients receiving thiazide diuretics, hypersensitivity reactions may occur even in the absence of a history of allergic reactions or bronchial asthma.
Photosensitivity
Cases of photosensitivity reactions have been reported when taking thiazide diuretics. If photosensitivity occurs while taking hydrochlorothiazide, treatment should be discontinued.
Non-melanoma skin cancer and lip cancer
Two epidemiological studies based on the Danish National Cancer Registries showed an increased risk of developing non-melanoma skin cancer and lip cancer (basal cell carcinoma of the skin and squamous cell carcinoma of the skin) with increasing cumulative dose of hydrochlorothiazide.
Hydrochlorothiazide has a photosensitizing effect, which may cause the development of non-melanoma skin and lip cancer.
Patients taking hydrochlorothiazide should be informed of the risk of developing non-melanoma skin and lip cancer and the need to regularly examine the skin for new changes as well as changes in existing ones. If any suspicious skin lesions are detected, the patient should immediately consult a doctor. Particular attention should be paid to patients who have known risk factors for skin cancer, including: skin phototypes II (pale and fair skin), a family history of skin cancer, a history of skin damage caused by sun or ultraviolet radiation and radiation therapy , smoking and taking drugs with photosensitizing effects.
Patients should be advised to take measures to prevent the development of skin cancer, such as limiting time in the sun and exposure to ultraviolet rays, and using appropriate sunscreens when exposed to the sun. Any suspicious skin lesions should be immediately examined, including histological examination of material obtained by biopsy of tissue at the site of the lesion. It may also be necessary to reconsider the use of hydrochlorothiazide in patients with a history of non-melanoma skin cancer and lip cancer.
Athletes
Hydrochlorothiazide may give a positive result during doping control in athletes.
Other
In patients with severe atherosclerosis of the cerebral and coronary arteries, hydrochlorothiazide should be used with extreme caution.
Thiazide diuretics can reduce the amount of iodine bound to plasma proteins without causing signs of thyroid dysfunction.
Evidence from epidemiological studies
Two epidemiological studies based on the Danish National Cancer Registries revealed a relationship between hydrochlorothiazide use and the risk of developing non-melanoma skin and lip cancer (basal cell carcinoma and squamous cell carcinoma). In one study, high-dose hydrochlorothiazide (cumulative dose >50,000 mg) was associated with the development of basal cell carcinoma and squamous cell carcinoma. Another study observed a possible association between the risk of lip cancer and hydrochlorothiazide use. There was a clear relationship between cumulative dose and response for patients who received at least one dose, for patients who received the highest dose (>25,000 mg), and for patients who received the highest cumulative dose (>100,000 mg).
Losartan
Angioedema
Patients with a history of angioedema (including swelling of the larynx and vocal folds with the development of airway obstruction and/or swelling of the face, lips, pharynx and/or tongue) require careful monitoring of the use of the drug.
Arterial hypotension and decreased circulating blood volume (CBV)
In patients with hypovolemia and/or reduced sodium levels in the blood plasma resulting from intensive use of diuretics, restriction of dietary salt intake, diarrhea or vomiting, symptomatic arterial hypotension may develop (especially after taking the first dose). It is necessary to correct such conditions before starting the use of losartan.
Water-electrolyte imbalance
Fluid and electrolyte imbalances often occur in patients with impaired renal function (with or without diabetes mellitus), therefore the concentration of potassium in the blood plasma and creatinine clearance should be carefully monitored, especially in patients with heart failure and creatinine clearance in the range of 30-50 ml /min. The simultaneous use of losartan with potassium-sparing diuretics, potassium supplements and potassium-containing salt substitutes is not recommended.
Liver dysfunction
Pharmacokinetic data indicate a marked increase in plasma concentrations of losartan in patients with cirrhosis; losartan should be used with caution in patients with a history of mild or moderate hepatic impairment (<9 Child-Pugh points). There is no experience with the use of losartan in patients with severe liver dysfunction, therefore the use of losartan is contraindicated in this group of patients.
Renal dysfunction
Impaired renal function has been reported due to inhibition of the RAAS, including renal failure (particularly in patients whose renal function is dependent on the RAAS, for example, with severe heart failure or existing renal impairment). As with the use of other drugs that affect the RAAS, cases of increased concentrations of urea and creatinine in the blood plasma have been described in patients with bilateral renal artery stenosis or with renal artery stenosis of a single kidney. These changes in renal function may be reversible and decrease after treatment is discontinued. Losartan should be used with caution in patients with bilateral renal artery stenosis or renal artery stenosis of a solitary kidney.
Kidney transplant
There is no experience with the use of losartan in patients who have recently undergone kidney transplantation, so caution should be exercised when using the drug in such patients.
Primary hyperaldosteronism
Patients with primary hyperaldosteronism typically do not respond to treatment with antihypertensive drugs that inhibit the RAAS. For this reason, the use of losartan is not recommended.
Coronary heart disease and cerebrovascular disease
As with the use of any other antihypertensive drugs, an excessive decrease in blood pressure in patients with coronary heart disease or cerebrovascular disease can lead to the development of myocardial infarction or ischemic stroke.
Heart failure
As with other drugs that affect the RAAS, patients with heart failure with or without renal impairment are at risk of developing severe hypotension and acute renal failure.
Aortic and mitral valve stenosis, hypertrophic obstructive cardiomyopathy
As with other vasodilators, special caution should be exercised in patients with aortic or mitral stenosis or hypertrophic obstructive cardiomyopathy.
Differences due to ethnicity
By analogy with other ACE inhibitors, losartan and other ARBs are markedly less effective in lowering blood pressure in blacks compared to patients of other races. This may be due to more frequent cases of low renin concentrations in representatives of the Negroid race with hypertension.
Dual blockade of the renin-angiotensin-aldosterone system
There is evidence that the simultaneous use of ACE inhibitors, ARB II or aliskiren increases the risk of arterial hypotension, hyperkalemia and renal dysfunction (including acute renal failure), therefore, double blockade of the RAAS when using a combination of losartan with ACE inhibitors or aliskiren is not recommended. If it is necessary to carry out double blockade of the RAAS, treatment should be carried out under the supervision of a specialist with frequent and careful monitoring of renal function, water and electrolyte balance and blood pressure indicators.
Concomitant use of ARB II, including losartan, with drugs containing aliskiren is contraindicated in patients with diabetes mellitus and/or patients with moderate to severe renal impairment (GFR less than 60 ml/min/1.73 m2 body surface area) and is not recommended in other patients (see section “Contraindications”),
Concomitant use of ARB II, including losartan, with ACE inhibitors is contraindicated in patients with diabetic nephropathy and is not recommended in other patients (see section "Contraindications").
Excipient
The drug contains Crimson dye [Ponceau 4R], which can cause allergic reactions.
Indications for use of the drug Lozap
Lozap : hypertension (arterial hypertension); reducing the risk of cardiovascular complications and mortality in patients with hypertension (arterial hypertension) and left ventricular hypertrophy; protection of kidney function with type II diabetes mellitus with proteinuria in order to slow the progression of kidney disease (preventing the need for dialysis and kidney transplantation), as well as to reduce proteinuria; chronic heart failure, if therapy with ACE inhibitors is inappropriate. Lozap Plus : hypertension (arterial hypertension) (patients for whom combination therapy is indicated); reducing the risk of developing cardiovascular complications and mortality in patients with hypertension (arterial hypertension) and left ventricular hypertrophy.
general description
Is as follows:
| Drug/Features | "Lozap" | "Lozap plus" |
| Release forms | Pills | Pills |
| Dosage | 12.5 mg | 62.5 mg |
| 500 mg | ||
| 100 mg | ||
| Appearance | An oblong, biconvex white tablet. A cardboard pack contains 30, 60 or 90 capsules | An oblong shape of a light yellow hue with a transverse dash. The package may contain 10, 20, 30 or 90 pills |
Use of the drug Lozap
For hypertension (arterial hypertension), the initial and maintenance dose is 50 mg 1 time per day. The maximum antihypertensive effect is achieved 3–6 weeks after the start of administration. In some cases, to achieve a greater effect, the dose is increased to 100 mg once a day. When prescribing the drug to patients with reduced intravascular volume (for example, receiving diuretics in high doses), a lower initial dose is recommended - 25 mg 1 time per day. No dose adjustment is required in elderly patients or patients with impaired renal function, including patients on dialysis. Patients with impaired liver function should be prescribed Lozap at a lower dose. The starting dose for patients with chronic heart failure is 12.5 mg once daily. In the future, the dose should be titrated, as a rule, gradually increasing it every week by 12.5 mg / day (i.e. 12.5; 25; 50 mg / day), reaching an average maintenance dose of 50 mg 1 time per day, depending on tolerability drug. The titration period is determined taking into account individual tolerability of treatment. The drug is taken regardless of meals; The tablet is swallowed without chewing, washed down with water.
Composition and release form
The drug Lozap is available in the form of small tablets for parenteral administration. They are white, slightly elongated and convex on both sides. They have a soluble thin film shell. Packaged in blisters of 10 pieces. One cardboard package contains 3, 6, 9 blisters and includes instructions for use.
The active substance is potassium losartran.
Auxiliary components: cellulose, povidone, talc, magnesium stearate, macrogol, dyes, mannitol, croscarmellose sodium.
Side effects of the drug Lozap
May occur in the form of anaphylactic reactions, angioedema, including swelling of the larynx and glottis, with the development of airway obstruction and/or swelling of the face, lips, pharynx and/or tongue. In controlled clinical trials, the only side effects were dizziness and hypotension. In some cases, patients receiving losartan experienced hepatitis, diarrhea, impaired liver function, migraine, myalgia, arthralgia, urticaria, and itching. Adverse reactions from the respiratory tract have been described: cough, upper respiratory tract infections. When treated with losartan, a dry cough is detected.
Side effects
As a rule, during the course of therapy, patients experience virtually no side effects. If they appear, they go away on their own and quickly, so there is no need to discontinue the drug. The following side effects are possible when taking Lozap:
- Dizziness, increased fatigue, headache, problems falling asleep. Migraines, anxiety, tremor, and depression are less common.
- Infection of the respiratory system. Signs of rhinitis, bronchitis and respiratory distress may appear.
- Dyspeptic symptoms, rarely gastritis, dry mouth, flatulence.
- Disturbance of the musculoskeletal system. Possible pain in the back and muscles, cramps.
- Signs of cardiac dysfunction are expressed in tachycardia, bradycardia, arrhythmia.
- Rarely, kidney problems, sexual dysfunction and infections of the urinary system appear.
- Allergic reactions, dry dermis, excessive sweating.
Special instructions for the use of the drug Lozap
Therapy with Lozap is not prescribed to patients with a deficiency of intravascular fluid volume (for example, patients receiving diuretics in high doses). If you have a history of liver disease, you should consider using the drug at a lower dose. In the presence of acute or chronic renal failure, the drug may lead to deterioration of renal function with or without hyperkalemia. Lozap should be used with caution in patients with bilateral renal artery stenosis or renal artery stenosis of a solitary kidney. Clinical studies have not revealed age-related differences regarding the effectiveness or safety of the drug. The use of the drug may negatively affect activities that require a high speed of mental and physical reactions (for example, when driving vehicles, servicing machines and mechanisms, working at heights, etc.).
Combination with other drugs
Interaction with other antihypertensive medications leads to an enhanced therapeutic effect. “Lozap” and “Lozap plus” can be combined with other drugs for the treatment of hypertension and heart failure.
Taking Lozapa Plus together with potassium-sparing diuretics is undesirable, as hyperkalemia may occur.
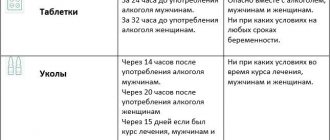
Not everyone knows the difference between Lozap and Lozapa Plus. Both described drugs are prohibited from being combined with alcohol, since such a combination can lead to a decrease in blood pressure. In this case, the person will experience nausea, vomiting, dizziness, numbness of the limbs, and impaired coordination of movements. He may feel generally unwell.
If taking Lozapa Plus is combined with drinking alcoholic beverages, you may notice a decrease in the therapeutic effect of the drug. It contains a diuretic component. When combined with alcohol, urination increases, and accordingly, the concentration of the active substance decreases.
If the patient has previously had angioedema, then throughout the entire therapy with the described drugs, medical supervision should be exercised, since a relapse of a severe allergic reaction is possible.
If a patient is diagnosed with hypovolemia or hyponatremia, caused by various factors, then hypotension may develop when taking Lozap and Lozap plus. If these disorders are present, before starting therapy with the described drugs, it is necessary to eliminate disturbances in the water-electrolyte balance or take both drugs in minimal dosages.
Drug interactions Lozap
In clinical and pharmacological studies, no clinically significant interactions were observed with hydrochlorothiazide, digoxin, warfarin, cimetidine, phenobarbital, ketoconazole and erythromycin. Rifampicin and fluconazole reduce the level of the active metabolite of losartan. The clinical consequences of these interactions have not been assessed. Strengthens (mutually) the effect of other antihypertensive drugs (diuretics, β-adrenergic receptor blockers, sympatholytics, other drugs that block ACE). Increases the risk of hyperkalemia when combined with potassium-sparing diuretics (for example, spironolactone, triamterene, amiloride) and drugs containing potassium or its salts. NSAIDs, including selective COX-2 inhibitors, reduce the effect of diuretics and other antihypertensive drugs. Therefore, the antihypertensive effect of ACE II receptor antagonists may be reduced by NSAIDs, including COX-2 inhibitors. The severity of the hypotensive effect of losartan, like other antihypertensive drugs, can be reduced with the help of indomethacin.
Lozap overdose, symptoms and treatment
In case of overdose (intoxication) of the drug, symptoms such as hypotension, tachycardia may appear, and sometimes bradycardia may occur due to parasympathetic (vagal) stimulation. If symptomatic hypotension occurs, maintenance therapy is provided. In case of accidental overdose (taking the drug in a high dose), it is necessary to carry out symptomatic and supportive therapy, induce vomiting and gastric lavage. Neither losartan nor its active metabolite can be removed by hemodialysis.
Therapeutic properties
Indications for the use of the drug "Lozap" are different. The drug will allow:
- Reduce blood pressure and keep it normal.
- Reduce the load on the heart.
- Reduce the amount of aldosterone and adrenaline in the blood.
- Increase tolerance to physical and emotional stress in people with cardiovascular diseases.
- Improve cardiac circulation and renal blood flow intensity.
A moderate diuretic effect is also possible from taking the drug.
Within a few hours you can notice the first positive effect from taking the capsule. It will keep throughout the day. For a sustained reduction in blood pressure, the therapeutic course should be 1 month.
The drug is particularly effective in treating those with malignant arterial hypertension.
“Lozap Plus”, in addition to the described therapeutic actions, produces additional:
- Helps reduce the concentration of potassium in the blood.
- Activates the production of the hormone renin.
- Reduces the concentration of uric acid and accelerates its elimination.
The active substances of the drugs are perfectly absorbed by the body and quickly enter the bloodstream from the gastrointestinal tract.