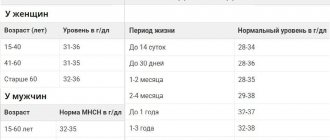
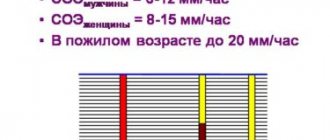
© Author: Z. Nelly Vladimirovna, laboratory diagnostics doctor at the Research Institute of Transfusiology and Medical Biotechnology, especially for SosudInfo.ru (about the authors)
The term “macrocytosis” refers to a phenomenon in which large quantities of erythrocytes (red blood cells) are present in the blood, slightly or significantly changing their size towards an increase. Anemic syndrome, caused by the presence of a large number of enlarged formed elements of the erythrocyte series, is classified as macrocytic anemia.
Macrocytosis is detected by an automatic analyzer (erythrocyte indices MCV and RDW), and then by a doctor in a stained blood smear when studying the morphological characteristics of red blood cells.
Cells with a diameter of 8 microns and above fall into the category of macrocytes (the diameter of healthy red blood cells is ≈ 7-8 microns - normocytes, everything below is microcytes).
Meanwhile, in certain pathological conditions (lack of vitamin B12 and folic acid, for example), cells appear in the blood that are larger in size than macrocytes, their diameter is more than 10 microns - these are megalocytes . The anemia that results from this will also be macrocytic, but more often it is called megaloblastic in order to emphasize its origin. It should be borne in mind that not all macrocytic anemias are megaloblastic; in other pathological conditions caused by other reasons, red blood cells do not increase to such enormous sizes and remain macrocytes.
Enlarged cells usually carry a larger amount of red blood pigment, chromoprotein - hemoglobin, so their color may be more intense than those red blood cells that are saturated with hemoglobin correctly or even less than necessary. This intense staining of macrocytes is called hyperchromia. Macrocytosis with hyperchromia are the main laboratory signs of hyperchomic macrocytic anemia.
blood is normal and with hyperchromic macrocytic anemia
Macrocytosis of erythrocytes in a general blood test
The key point in the diagnostic search (in relation to macrocytic anemia) is a general blood test (hemogram), or rather, its individual parameters:
- Morphological characteristics of red blood cells (detection of macrocytes, poikilocytosis);
- MCV indicator (mean blood cell volume) - it shows values above 120 femtoliters with macrocytosis of erythrocytes;
- Hematocrit level (in severe vitamin deficiency anemia for a long time, the hematocrit drops to 30-25%, although in other forms of macrocytic anemia it may remain within normal values).
It should be noted that the nature of the process is significant, since it is the chronic course of the pathology that creates the preconditions for the disappearance of normal red cells and their replacement by macrocytes.
In patients suffering from anemic syndrome for a shorter period of time, the indicator may only slightly exceed the upper limit of normal values or even be within the normal range. Then you will have to take into account other circumstances that could create conditions for the development of macrocytic anemia. Macrocytosis, caused by the use of chemotherapy drugs or damage to the hepatic parenchyma, is usually mild or moderate. Reticulocytosis with a more or less uniform increase in red blood cells usually also does not raise doubts with the doctor. But with regard to vitamin deficiency conditions, questions always arise. However, the table below will help you compare and evaluate laboratory parameters for different conditions.
Table: options for increasing the size of red blood cells
| Pathological condition | MCV, fl | Morphological characteristics of cells |
| Megaloblastic anemia HCT (hematocrit) below 30% | 100 — 130 | Hyperchromia, macrocytes, poikilocytosis (ovalocytes, schizocytes) |
| Reticulocytosis (RET more than 10%) | 100 — 110 | Polychromatophilic elements - macrocytes (immature forms) |
| Lesions of the liver parenchyma | 90 — 110 | Macrocytes, uniform increase in cell diameter and volume (all red blood cells are approximately the same size) |
Macrocytosis caused by a lack of cyanocobalamin - vitamin B12, or folic acid - vitamin B9 (or both) has noticeable differences. When studying a smear morphologically:
blood for B12 deficiency anemia
- Poikilocytosis of erythrocytes;
- The presence of fragments of destroyed cells in the smear (schizocytosis);
- Hyperchromia;
- Changes in the “white” blood - a significant increase in the content of neutrophilic leukocytes, the nucleus of which has 5 or 6 segments, while normally the number of cells containing more than five segments in their nucleus is unlikely to reach 5% of the total number of segmented neutrophils .
The presence of a huge number of polysegmented neutrophil leukocytes is a kind of equivalent of poikilocytosis of red blood cells and is an important laboratory symptom of megaloblastic anemia.
Types of hematological studies
The main hematological study is a clinical blood test, the results of which reflect the general condition of the body and provide the doctor with information about the nature of hematopoiesis (blood formation).
The analysis is used to diagnose inflammatory processes, anemia, leukemia and many other pathological conditions. The study is prescribed to all patients who seek specialized medical care. It is also carried out during pregnancy, preventive examinations, and during medical examination.
The biological material for research can be capillary or venous blood. A clinical blood test consists of many tests (from 8 to 30). Some of these may be independent hematology studies.
Do unnaturally large red blood cells appear in the blood?
The appearance of abnormally large formed elements of the erythrocyte series and polysegmented neutrophils in a general blood test indicates, first of all, a disorder of hematopoiesis in the early stages, in the bone marrow (megaloblastic type of hematopoiesis). As a result of megaloblastic hematopoiesis in the bone marrow:
- Cell division is disrupted, at the stage of these processes the cells' nuclear structure, diameter and volume change, and as a result, they unnaturally increase in size (megaloblasts);
- Cells mature at different times - asynchronously: some are already close to mature forms, others have made little progress in their development and remain at the level of promyeloblasts;
- Megaloblasts begin to be prematurely saturated with chromoprotein - hemoglobin, fortunately, the red blood pigment of their increased volume is more than enough, there is somewhere to be located (provided that hemoglobin synthesis is not impaired);
- However, degenerative changes in the nuclei make many cells defective, unable to survive to a mature state.
Thus, ineffective erythropoiesis, “giving life” to giant cells, does not provide them with good “health”. Most of the elements that are destined by nature to become full-fledged red blood cells and perform important functions (transport oxygen and carbon dioxide, take part in metabolic processes, play the role of suppressors in immune reactions, etc.) simply die, leaving behind only fragments that will then circulate in the blood (schizocytosis), along with other formed elements.
Of course, not all cells will die at the maturation stage; some of them (the most persistent) will remain and enter the bloodstream - in a general blood test they will be represented by abnormally enlarged, mainly hyperchromic, erythrocytes-macrocytes (erythrocyte macrocytosis). In addition, fragments of “former” (dead) red blood cells (schizocytes) will be detected in the erythrogram, creating a picture of poikilocytosis and suggesting the development of hyperchromic macrocytic anemia. However, for a more accurate diagnosis, additional research will be needed.
In addition to macrocytosis of erythrocytes in a general blood test, macrocytic morphological changes in bone marrow aspirate and the level of vitamins in the blood should be taken into account.
To prevent the diagnostic search from going down the wrong path, other possible prerequisites for the disease must be studied and taken into account:
- Medical history and previous pathology;
- Family, social, professional, medicinal history;
- Examinations of the head and neck, cardiovascular and nervous system, respiratory system and abdominal cavity.
All these diagnostic criteria are necessary to establish the etiology and form of macrocytic anemia.
Reasons for their appearance
In general, macrocytosis of erythrocytes is not an independent nosological entity, it is a laboratory symptom indicating another pathology. The cause of such metamorphoses that occur with red blood cells may be conditions that disrupt the normal course of events in the process of maturation of red blood cells in the bone marrow or their increased destruction accompanying some pathological condition:
- Vitamin B12 deficiency is a hereditary or acquired deficiency of cyanocobalamin (vitamin B12), which causes the formation of hyperchromic megaloblastic (B12-deficiency) anemia;
- Folate deficiency (vitamin B9) – a lack of folic acid in the body threatens the development of folate deficiency anemia (this is also hyperchromic macrocytic anemia);
- Combined variant - B12-folate deficiency anemia (medicine encounters this form most often);
- Anemic syndrome, the development of which is caused by acute blood loss (the compensatory mechanism is activated, but the red cells do not have time to become full-fledged red blood cells with normal diameter and volume);
- Certain types of hemolytic anemia - increased breakdown of red cells in blood vessels or tissues triggers intense but ineffective erythropoiesis in the bone marrow, as a result - in a general blood test, poikilocytosis (schizocytosis), macrocytosis of erythrocytes, and other signs of breakdown of blood cells can be observed;
- Myelodysplastic syndrome, in which various changes in the general blood test are generally possible;
- Some forms of leukemia;
- Pre-leukemic conditions (idiopathic sideroblastic anemia, Di Guglielmo syndrome - acute malignant erythromyelosis);
- Decreased functional capacity of the thyroid gland (hypothyroidism);
- Severe long-term intoxication in chronic alcoholism;
- Damage to the liver parenchyma, which creates reserves of various vitamins (including cyanocobalamin and folic acid), which are subsequently assigned to participate in the synthesis of purine and pyrimidine bases, and they are known to be necessary for the production of complete DNA;
- The use of certain medications: inhibitors of dehydrofolate reductase (triamterene, chloridine, methotrexate), pharmaceuticals that affect the metabolism of purines and pyrimidines (allopurinol, febuxostat), as well as antiepileptic drugs and oral contraceptives - all of them can disrupt DNA synthesis and cause the development of macrocytic anemia ;
- Malignant neoplasms that disrupt cell division and DNA formation;
- Diseases of the gastrointestinal tract and surgical interventions on the digestive organs;
- Pregnancy (during this period, hematopoiesis occurs in an active mode, vitamins received and accumulated are also consumed intensively, which is why folate deficiency anemia often forms during this period).
Due to the fact that B12 and folate deficiency conditions are first on the list of causes, I would like to draw the reader’s attention to the complex functional relationship between these vitamins, which creates conditions for disruption of the entire process of DNA formation. A lack of vitamin B9 in food very quickly reduces the ability to demethylate and bind to cyanocobalamin individual folates that accumulate in the liver, resulting in impaired DNA production. With a lack of vitamin B12 in food, similar disorders occur and the result is also similar - DNA synthesis suffers.
general characteristics
Most of the human blood contains red blood cells - erythrocytes. They are responsible for transporting oxygen to tissues. Red blood cells must maintain their shape and size throughout their life. Red blood cells are biconcave discs measuring 7 to 8 microns in size. Each normal red blood cell can carry about 300 million hemoglobin molecules. In some diseases, especially anemia, changes in the size and shape of red blood cells are observed. Most often, they become smaller and can no longer properly supply tissues with oxygen. If the size of red blood cells is less than 6 microns, they are called microcytes.
There are different types of red blood cells in human blood - the presence of a small number of altered red blood cells is considered normal. Microcytosis in a general blood test is diagnosed when there are many such cells - more than 25%. Most often, this condition indicates the development of microcytic anemia and requires special treatment.
Important: this laboratory indicator appears in some pathological conditions and is an important diagnostic criterion. After all, such red blood cells are not able to carry hemoglobin and do not perform their functions.
In this case, several variants of reduced red blood cells are detected in the blood. These are actually microcytes - cells that are less than 6 microns in size, but do not change in shape. In addition, if red blood cells, in addition to decreasing in size, lose their biconvex shape and become spherical, they are called microspherocytes. Sometimes fragments of red blood cells or their fragments, 2–3 microns in size, are also detected in the blood. These are schizocytes.
An increase in the number of these altered red blood cells can have varying degrees of severity:
- with moderate microcytosis, no more than 40% of microcytes are detected;
- if pathological cells from 40 to 70% are diagnosed with an average severity of pathology;
- when the number of microcytes is more than 70%, severe microcytosis is diagnosed.
Changes in the size of red blood cells are an indicator of many pathologies. This condition is called anisocytosis, and microcytosis is one of its varieties. The results of such tests are recorded on a blood test form with the designation RDW.
The results of the study of the size of red blood cells are indicated by the letters RDW.
But the study of the size of red blood cells is not always carried out. Indications for such an analysis may include frequent unreasonable increases in body temperature, heavy sweating, sudden mood changes, decreased performance, lethargy and drowsiness. If you complain about this condition, the doctor prescribes an RDW test.
Prevalence
The prevalence of macrocytic (megaloblastic) anemia may depend on various factors:
- Nutritional characteristics of certain categories of people;
- Gastrointestinal pathology, common in a particular human population, and the number of surgical interventions on the digestive organs undergone;
- The use of drugs that interfere with the metabolism of folic acid, purine and pyrimidine bases and thus affect the quality of DNA synthesis;
- Prevalence of neoplastic processes in certain geographic areas.
At the same time, the leading prerequisites for the formation of macrocytic anemia in Russia and Western European countries primarily include hereditary or acquired disorders associated with deficiency of vitamin B12 and folic acid.
As statistics show, very often acquired macrocytic anemia develops in conditions that seem to be mutually exclusive - due to alcoholism or during pregnancy. In this regard, I would like to inform the reader of some interesting (in our opinion) facts.
Alcoholics don't always take risks
In alcoholism, megaloblastic anemia develops during a long binge, spanning several weeks. This happens because in most cases, alcoholics, carried away by the search for alcohol, completely forget about food, and this leads to depletion of vitamin B9 reserves in the body (true deficiency). Alcohol negatively affects metabolic processes designed to provide tissues with folate, and constant drunkenness, or rather chronic alcoholism, does not allow folic acid to take part in the intestinal-hepatic cycle, which reduces its entry into the bone marrow. As a result, bone marrow hematopoiesis is disrupted, and hyperchromic megaloblastic anemia develops. However, there is one “but”...
If a person suffering from alcoholism does not neglect a normal “snack” and consumes vitamins in sufficient quantities with food (including folic acid and cyanocobalamin), then bone marrow hematopoiesis continues to proceed normally and anemic syndrome does not develop.
The fetus has more privileges
And regarding pregnancy...
It should be noted that the child has more privileges than the mother regarding the consumption of vitamins involved in DNA synthesis. The fact is that the placenta, protecting the baby, extracts the incoming amount of folate and takes it upon itself, without “sharing” much with the mother’s body.
A lack of folic acid in the food of a pregnant woman will most likely not affect the development of the baby - the placenta will “take care” and extract the required amount to the detriment of the mother’s body, but the mother herself must think about herself and calculate her diet so that it contains enough benefits for her substances.
Vitamin B12 deficiency, on the contrary, is unlikely to threaten a woman during pregnancy, much less a fetus. If the reserves of folic acid contained in the liver are enough for 2-3 months, then cyanocobalamin can be consumed for 2-3 years painlessly, the main thing is that in both the first and second cases the liver parenchyma must be healthy.
Start by eliminating the cause
Macrocytosis of erythrocytes itself, of course, is not treated, because it is just a symptom identified in a general blood test. Treatment begins with eliminating the cause that created the formation of large cells. Meanwhile, it is not always possible to quickly eliminate the culprits of the misfortunes that have befallen them. Then long-term therapy begins for the doctor and the patient, aimed at the underlying pathology that caused the development of macrocytic anemia.
With vitamin deficiency conditions, everything is more or less clear; they are treated with appropriate medications (medicinal forms of cyanocobalamin and folic acid). However, if acquired deficiency (lack of food, malabsorption in the intestines, the influence of alcohol, competitive absorption by helminths, etc.) is easily amenable to therapeutic influence, then congenital anomalies react poorly to treatment, moreover, they are often accompanied by mental retardation and other abnormalities (megaloblastic anemia in children). Here we have our own tactics.
As for the entire list of diseases that gave rise to the formation of abnormally enlarged red blood cells in the bone marrow or to their premature and intense breakdown in the blood, in each case there is a separate approach: in some cases blood transfusions (blood transfusions) will help, in others they will be required surgical intervention.
Unfortunately, it is not only quite difficult, but also impossible, to describe all the options for the treatment process, however, readers can find answers to their questions regarding certain types of macrocytic anemia in the relevant publications posted on the pages of our website.
How it manifests itself
People with elevated levels of microcytes in the blood do not have specific symptoms. When feeling unwell, weak and decreased in performance, not everyone even goes to the doctor. But the severity of microcytosis depends not on its degree, but on its duration.
Attention: without timely treatment, symptoms will only get worse. Changes in blood composition greatly affect a person’s health.
Oxygen starvation and impaired blood composition are manifested by the following external signs:
- weakness, drowsiness;
- disturbance of taste sensations;
- dry mouth, seizure formation;
- atrophy of the papillae of the tongue, tingling, change in its color;
- frequent nausea, urge to vomit;
- sensation of a lump in the throat, difficulty swallowing;
- pale and dry skin;
- dry and brittle hair and nails;
- shortness of breath, tachycardia;
- itching of the external genitalia.
A person with microcytosis experiences headaches, dizziness, severe shortness of breath after exercise, and may even lose consciousness. If this condition is observed in pregnant women, swelling appears, and the child suffers from hypoxia.
With prolonged microcytosis, all tissues of the body experience oxygen starvation. At the same time, the functioning of the respiratory and cardiovascular systems can be disrupted, immunity decreases, and in children, physical and mental development slows down.