An important anatomical component of the heart is the valve apparatus. Without it, blood would not be able to move in one direction, which is why it is extremely important that all valves are in good condition and functioning correctly. Variants of the norm and physiological characteristics of the heart valve apparatus will be considered.
Heart valves are necessary for the portioned ejection of blood during contraction of the heart. Their main function is to prevent backflow of blood (regurgitation) and ensure that it always moves in the same direction through the heart. The closure of heart valves can usually be heard with a stethoscope, which can be used for the initial diagnosis of valvular conditions.
Video: Structure of the human heart, blood circulation circles
Description
All heart valves are covered with endothelium. The three layers that form the basis of the valve apparatus have specific characteristics and are called fibrosa, spongiosa and ventricularis. During heart contractions, spongiosa, rich in glycosaminoglycans, facilitates the process of rearrangement of collagen and elastic fibers.
Vacular interstitial cells (VICs) are abundant in all layers of heart valves and contain a variety of dynamically targeted components. The regulation of collagen and other structural components is provided by enzymes synthesized by VIC. The integrity of valve tissue is maintained by the interaction of valve endothelial cells (VECs) with the VIC. Changes and remodeling of the valvular interstitial and endothelial structure contribute to disruption of the valve properties, and subsequently valve function.
Basics of proper operation of the valve apparatus:
- The valves are properly formed and flexible.
- The valves open completely, allowing the required amount of blood to pass freely through the opening.
- The valves close tightly, then blood does not flow back
Causes of heart valve defects
Heart valve defects in adults are diseases that are based on disorders of the valve apparatus (valve leaflets, annulus fibrosus, chordae, papillary muscles), congenital or developed as a result of diseases and injuries, disrupting proper blood flow through the valves and leading to serious complications, such such as severe heart failure, syncope, arrhythmias, sudden cardiac death, etc.
Stenosis is a narrowing of the valve opening for various reasons, as a result of which the heart has to work excessively to overcome this obstacle.
Valve insufficiency is a malfunction of the valve leaflets, leading to their incomplete closure and the return of blood back into the heart chamber, which leads to the heart working with excess blood volume.
Aortic valve
The tricuspid valve, located at the mouth of the aorta, separates the cavity of the left ventricle from the aorta. Behind the three semilunar cusps (right coronary, left coronary and posterior non-coronary) of the aortic valve are dilated pockets of the aortic ostium, called sinuses of Valsalva. The right coronary artery arises from the right coronary sinus, and the left coronary artery arises from the left coronary sinus. The area where all three valves meet is called the commissure.
The opening and closing of the aortic valve is a passive pressure-controlled mechanism, unlike the mitral valve.
The tissue of the aortic valves is stretched as a result of counteraction during diastole, and elastin elongates and stretches. Therefore, normally the aortic valve leaflets are quite flexible and durable, able to withstand systemic pressure. During the systole phase, the release of elastin ensures relaxation and shortening of the leaflet. Optimal valve function requires perfect alignment of the three return points.
Associated diseases: aortic regurgitation (also called aortic regurgitation), aortic stenosis.
Functions of the mitral snort
This leaflet heart valve is located in the left chamber between the ventricle and atrium. When open, it performs the function of being the entrance for blood flow into the ventricle. When the heart muscle is in the systolic phase, the valve blocks the backflow of blood.
The medical history of the field of cardiology indicates that due to its structure, the mitral snort (bivalve) is the first to be recognized on ultrasound. Due to its anatomy, it reflects the ultrasound signal well. Due to the fact that the anterior valve of the snort has good plasticity and mobility, medical specialists can examine in detail the structure of the valve apparatus.
Mitral valve
The mitral valve was named after the mitre by Andreas Vesalius (De Humani Corporis Fabrica, 1543). This valve is located at the junction of the left atrium and the left ventricle. Its structure consists of five functional components:
- doors;
- annular space;
- chordae tendineae;
- papillary muscles;
- nearby myocardium.
The annulus fibrosus is an area of connective tissue containing discontinuous fibrous and muscle fibers that connect to the left atrium and ventricle. The anterior valve covers about one-third of the primary fibrous anterior part of the ring. Part of the anterior leaflet of the mitral valve is located in close proximity to the annular opening of the aortic valve. The ventricular, posterior, leaflet is attached to the posterior muscular half and two-thirds of the annular space. Due to the asymmetrical leaflets, the opening of the mitral valve is shaped like a funnel.
Chords from both the anterior and posterior papillary muscles are attached to each valve. The papillary muscles contract and extend the chordae during systole, which in turn promotes the closure of the mitral valve leaflets.
The mitral valve complex is separately distinguished, including the mitral valve and the left atrioventricular myocardium, endocardium and part of the aorta. This formation promotes the outflow of blood from the left ventricle. The forced passage of blood through the valve, as well as its tight closure during systole, is ensured by the coordination of the actions of the mitral-valve complex.
Associated diseases: mitral valve prolapse, mitral valve regurgitation, mitral valve stenosis.
Diagnosis of heart valve defects
Often, patients learn about problems with heart valves after a full, adequate examination by a doctor, who, during auscultation, identified a heart murmur, after which the patient is prescribed a number of tests that have different diagnostic value:
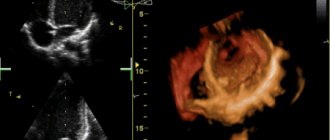
- transesophageal echocardiography (more complex and more expensive study);
- ECG;
- transthoracic echocardiography (ultrasound of the heart) is the most informative, common and inexpensive way to diagnose pathology of the heart valve apparatus;
- aortoventriculography;
- chest x-ray;
- multislice computed tomography with contrast.
At the initial stage of the disease, the patient may be prescribed medications that help the heart compensate for the excessive load due to valve disease. The selection of optimal therapy in this case should be carried out by an experienced cardiologist. However, heart valve disease is a problem that over time may require surgery to repair or replace the damaged valve.
Indications for heart valve replacement surgery:
- progressive heart failure;
- hemodynamically significant valve lesions;
- ineffectiveness of drug therapy;
- risk of severe complications.
Surgical treatment: heart valve replacement
In recent years, significant progress has been made in the surgical treatment of heart valves. Improvements in technology (including artificial blood circulation machines), the development of uniform standards and protocols for both preoperative examination and the course of the operation have made it possible to reduce the risks of perioperative complications, making the operation on the heart valve apparatus safer than refusing surgery and trying to live with valve dysfunction.
There are basically two types of heart valve surgery:
- prosthetics with artificial or biological prosthesis,
- reconstructive interventions.
It is quite natural that a person’s own valve, after successful reconstruction, functions better than an artificial prosthesis.
Reconstruction of the valve apparatus
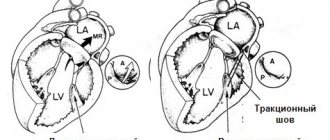
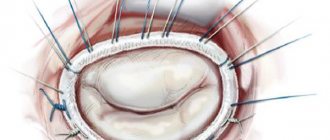
The purpose of valve repair is to eliminate the cause of its dysfunction. One of the options for plastic surgery of the mitral valve in case of mitral insufficiency is the removal of part of its posterior leaflet with subsequent annuloplasty or only annuloplasty (strengthening the fibrous ring of the valve using special support rings or reducing the diameter of the fibrous ring using special sutures - plastic according to De Vega, according to Batista, according to Alfieri).
In case of prolapse of the anterior leaflet of the mitral valve, it is possible to perform prosthetic replacement of the anterior leaflet chords, which normally ensure tight closure of the mitral valve. In case of aortic insufficiency, it is possible to perform an operation to normalize the closure of the valve leaflets - plastic according to El-Khoury. In case of valvular stenosis and the absence of calcification of the leaflets and fibrosis of the leaflets and subvalvular structures, it is possible to perform an open commissurotomy (separation of the areas of fusion of the valve leaflets).
Pulmonary valve
Also known as the pulmonary valve. The structure of the pulmonary valve is similar to that of the aortic valve. The valves have a semilunar shape; normally there are three of them (anterior, left and right). Similar to the valves, the sinuses are called sinuses, which are united with the pulmonary trunk through an arched ring (sinotobular junction). Like other valves, the pulmonary valve also has a fibrous ring and a commissure.
Associated diseases: pulmonary valve stenosis, pulmonary valve regurgitation.
Tricuspid valve
Also known as the tricuspid valve. Located in the right half of the heart at the junction of the atrium and ventricle. Consists of 3 valves, chordae tendons (anterior, posterior) and the often identified third papillary muscle. The tricuspid valve does not have a clearly defined collagen ring. The three flaps are attached to an elliptical shaped fibrous ring. The direct attachment of the cuspid septum is a hallmark of the tricuspid valve. Prominent papillary muscles support the valves in the commissures.
Normal valve function requires structural integrity and coordinated interactions between multiple anatomical components. Various pathophysiological mechanisms can cause heart valve disease.
Associated diseases: tricuspid atresia, tricuspid regurgitation, tricuspid stenosis.
Symptoms
Often, heart valve defects do not appear clinically for a long time, and complaints depend on the severity of the disease. When the disease manifests itself, patients experience shortness of breath, dizziness and fainting during exertion, a feeling of heaviness, chest pain, heart rhythm disturbances (arrhythmias), swelling, fatigue, and decreased performance. Often the heart’s ability to compensate for defects lasts for a long time. Therefore, patients seek help at a time when it is already difficult to help them due to the “neglect” of the disease, when the heart has exhausted its compensation capabilities and has turned, figuratively speaking, into an “overinflated balloon.”
Operation of the valve apparatus
In normal condition, the valves function in strict order, which allows the chambers of the heart to contract correctly and eject blood in the required volume. There are four main stages in the operation of the valve apparatus:
1. The atrioventricular valves (mitral and tricuspid) open, as a result of which blood rushes from the upper parts of the heart to the lower ones.
2. When the ventricles are filled, the pressure in their cavity increases, as a result of which the valves close. When the ventricles contract, blood fills the atria again (venous - right and arterial - left).
3. The aortic and pulmonary valves open. This also occurs under pressure when the ventricles contract and blood is pushed into large vessels and follows either to the lungs (from the right ventricle) or to all organs and tissues (from the left ventricle).
4. During relaxation of the ventricles, the pulmonary and aortic valves close. At this time, the atrioventricular valves open and blood again enters the ventricles from the atria for the next release into the bloodstream.
Types of valves used in prosthetics
Biological valves
They can be made from animal or human tissues (heterografts, homografts, autografts). Biological valves may contain some artificial components to provide valve support and placement. The main advantage of such a valve is that there is no need for lifelong anticoagulant therapy (constant strict use of drugs that significantly thin the blood and require constant blood tests), and the main disadvantage is its limited service life (10-15 years).
Mechanical valves
They consist entirely of mechanical elements (titanium and pyrolytic carbon) and are designed to replace the patient's own valve functions. The mechanical valve is very reliable and durable, designed for many years of full-fledged operation, which is the main advantage, but requires the patient to constantly take anticoagulants.
The Center for Cardiac Surgery and Cardiology provides assistance to patients with valvular pathology of varying complexity, including one-, two- and three-valve replacement with biological and mechanical prostheses of Russian and foreign production, elimination of valvular insufficiency using a variety of plastics (plasty on a support ring, tri- and quadriangular resection leaflets with annuloplasty according to De Vega, Batista) of the valve apparatus, restoration of the chordal apparatus by prosthetics of the mitral valve chords, etc. The main direction in surgery of valve pathology is aimed at increasing the number of reconstructive operations on the valve apparatus and reducing valve replacement.
The Clinic offers surgical treatment of heart valves in combination with other diseases, such as coronary heart disease, atrial fibrillation (atrial fibrillation).